and Peter S. Conti2
(1)
Department of Radiology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
(2)
Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
Prostate Cancer
Case 11.1
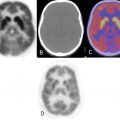
An 81-year-old male with metastatic adenocarcinoma of prostate, status postradiation therapy, presenting with widespread osseous metastatic disease involving predominantly T4–T7 vertebral bodies along with posterior ribs from T4–T6, likely representing epidural disease with perineural spread (Fig. 11.1). There are also small lesions involving the right lamina T10, proximal right 9th and 10th ribs, L-4 vertebral bodies, and bilateral posterior ilium.

Fig. 11.1
Case 11.2
A 75-year-old male diagnosed with metastatic adenocarcinoma of prostate, presenting with multiple foci of hypermetabolic and sclerotic osseous lesions involving L1, L3, right posterior L4, T12, and left T9 vertebral bodies (Fig. 11.2). Also noted is activity with faint sclerosis in the right anterior iliac bone and posterior left acetabulum.

Fig. 11.2
Case 11.3
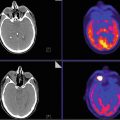
A 73-year-old male with history of prostatic adenocarcinoma, presenting with multiple hypermetabolic, predominantly sclerotic osseous lesions i nvolving the left temporal bone, right occipital bone, L1 vertebra, spinous process of L2, left iliac bone, and right iliac bone (Fig. 11.3).

Fig. 11.3
Case 11.4
A 64-year-old male with biochemically recurrent prostate cancer, post radical prostatectomy, and EBRT, presenting with faintly sclerotic but intensely hypermetabolic right L2 metastatic lesion (Fig. 11.4). Tc99m MDP bone scintigraphy was negative. Other nonneoplastic findings include T11 osteophytic activity, Paget’s-related increased right hemipelvis activity, and degenerative changes in the knees.

Fig. 11.3
Breast Cancer
Case 11.5
A 54-year-old female with breast cancer presenting with hypermetabolic, predominantly sclerotic osseous lesions noted in T11, right C7 lamina, inferior L4 and sacral promontory, several ribs, left posterior pillar of acetabulum, and right posterior iliac disease (Fig. 11.5).

Fig. 11.5
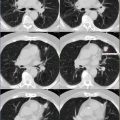
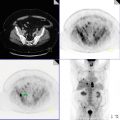
Case 11.6
A 68-year-old female with history of metastatic right breast carcinoma, post right lumpectomy with axillary lymph node dissection, and right lung VATS procedure with talc pleurodesis, presenting with several hypermetabolic osseous lesions seen predominantly in the pelvis and spine (Fig. 11.6). The purely blastic lesions are less avid, and the mixed lytic and sclerotic lesions demonstrate more intense metabolic activity. Mixed lytic and sclerotic lesions are seen at the posterior aspect of the right iliac bone, sacrum, and T8 vertebral body.

Fig. 11.6
Case 11.7
A 67-year-old female with history of metastatic breast cancer presenting with numerous osseous metastatic lesions involving the sternum, multiple ribs, L1 vertebral body, and left distal humerus (Fig. 11.7).

Fig. 11.7
Lung Cancer
Case 11.8
A 25-year-old male with history of metastatic squamous cell carcinoma of the lung presenting with several hypermetabolic, predominantly lytic lesions involving multiple levels of the cervical, thoracic, and lumbar spine, manubrium and sternum, multiple ribs bilaterally, scapulae, bilateral iliac bones, sacrum, acetabulae, and ischial and pubic bones (Fig. 11.8). There is sparing of the osseous structures of the upper and lower extremities bilaterally.