and Clarisse Dromain2
(1)
Department of Radiology, San Giovanni Hospital, Roma, Italy
(2)
Department of Radiology, Institut de Cancerologie Gustav Roussy, VilleJuif – Paris, France
Abstract
Fat stranding represents important CT findings leading radiologist attention to the site of abdominal pathology especially in patients presenting with acute abdominal pain. Fat stranding refers to an abnormal increased attenuation in fat (in the mesentery, omentum, retroperitoneum, or subcutaneous fat).
Fat Stranding
Fat stranding represents important CT findings leading radiologist attention to the site of abdominal pathology especially in patients presenting with acute abdominal pain. Fat stranding refers to an abnormal increased attenuation in fat (in the mesentery, omentum, retroperitoneum, or subcutaneous fat).
The underlying pathophysiologic process is increased edema and engorgement of lymphatics. Abdominal fat stranding can produce various appearances:
Ground–glass pattern due to mild inflammation (subtle hazy increased attenuation of the fat).
Reticulonodular pattern due to more severe inflammation (linear areas of increased attenuation.) A reticulonodular appearance can also be observed frequently in association with neoplastic disease (fat infiltration or peritoneal carcinomatosis).
Fat stranding is not a specific sign of a certain disease since it may occur in several conditions (appendicitis, cholecystitis, colitis, Crohn’s disease, diverticulitis, epiploic appendagitis, enteritis, infiltrative carcinoma, intestinal vasculitis, mesenteric ischemia, omental infarction, omental cake, panniculitis, pancreatitis, pelvic inflammatory disease, peritoneal carcinomatosis, urologic disease, and other less common conditions). Therefore it is essential to search other findings in the region where fat stranding is present in order to reach the correct diagnosis.
Fat Notch Sign
Fat notch sign is a recently described CT finding occulting in case of small bowel obstruction due to adhesive band. Fat notch sign corresponds to the extrinsic compression of the bowel at the transition zone by an extraluminal adhesive band (Fig. 1).
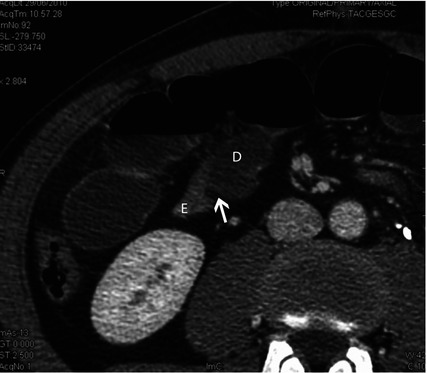
Fig. 1
The image shows a detail of a CT scan in a patient with mechanical small bowel obstruction due to adhesive band. D dilated small bowel loop, E empty small bowel loop, the arrow indicates the transition zone with the evidence of fat notch sign
Fecal Calprotectin Protein
Fecal calprotectin protein is a biochemical surrogate marker of chronic inflammatory bowel disease. It is a calcium- and zinc-binding protein with bacteriostatic properties abundant in neutrophil’s cytosol. It is resistant to enzymatic degradation and can be easily measured in feces. In inflammatory bowel disease patients, neutrophils influx into the bowel lumen leading to increases of fecal calprotectin. On the other hand, fecal calprotectin does not increase in patients with irritable bowel syndrome.< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


