Facet Joint Injection
Donald V. La Barge, III, MD
Key Facts
Terminology
Injection of corticosteroid and anesthetic into lumbar facet joint
Pre-Procedure
Facet joint osteoarthritis
Synovial cyst causing neurologic symptoms
Procedure
Prone
Angle C-arm or PA fluoroscopy tube slightly toward side of joint to be injected
Generally, lower 1/3 of joint is most amenable to needle entry/injection in arthritic joint
Ensure proper level
Slowly inject only enough contrast to confirm that needle tip is in joint space
Note pain scale and pain characteristics
Before, during, and after injection
Synovial cyst therapeutic rupture
May require significant injection pressure
See sudden spread of contrast into epidural space
Outcomes
Failure to alleviate pain
Wrong level injected
Injection extraarticular
Facet joint not the source of pain
May require multilevel injections
Most feared complications
Thecal sac puncture, cord injury, meningitis
Other complications
Nerve root injury, bleeding, infection
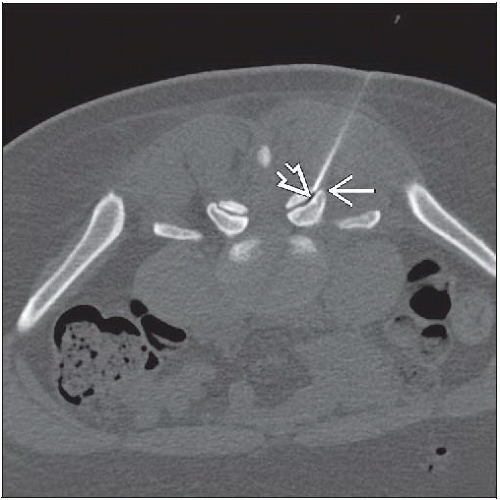 Axial NECT shows the needle tip  at the superolateral margin of the right L4/5 facet joint. Note that the needle is nearly within the plane of image and that the needle tip casts a dark artifact at the superolateral margin of the right L4/5 facet joint. Note that the needle is nearly within the plane of image and that the needle tip casts a dark artifact  . . |
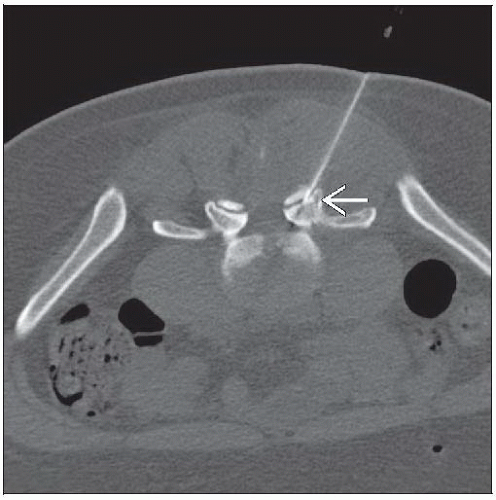 Axial NECT shows the needle tip  well seated within the right L4/5 facet joint. Imaging above and below to determine precise needle tip position is important with CT-guided interventions. well seated within the right L4/5 facet joint. Imaging above and below to determine precise needle tip position is important with CT-guided interventions. |
TERMINOLOGY
Abbreviations
Facet joint injection (FJI)
Synonyms
Facet joint injection = facet joint block
Facet = zygapophyseal joint
Definitions
Injection of corticosteroid ± anesthetic into lumbar facet joint
PRE-PROCEDURE
Indications
Facet joint osteoarthritis
Synovial cyst causing neurologic symptoms
Contraindications
Local or systemic infection
Coagulopathy
Allergy to injectate
Getting Started
Things to check
Imaging of facet joint for pathology and anatomic relationships
Informed consent
Laboratory: Coagulation parameters
Medications
Corticosteroid
Long-acting anesthetic (e.g., bupivacaine)
Short-acting anesthetic (e.g., lidocaine)
Myelography-safe iodinated contrast
Equipment list
Radiopaque marker
Sterile prep and drape materials
18-gauge drawing needles
5 mL syringe for local anesthetic with 1.5 inch 25-gauge needle
5-10 mL syringe for contrast with extension tubing
3 mL syringe for injectate
22-gauge spinal needle
Hydrogen peroxide
Sterile bandage
PROCEDURE
Patient Position/Location
Best procedure approach
Prone
Angle C-arm or PA fluoroscopy tube slightly toward side of joint to be injected
May need slight cranial angulation as well to optimize joint visualization
Generally, lower 1/3 of joint is most amenable to needle entry/injection in arthritic joint
Inferior recess may be only accessible site for injection in severely arthritic joint
Equipment Preparation
Draw ˜ 5 mL local anesthetic
Draw 5-10 mL myelography-safe iodinated contrast
Attach extension tubing and preload with contrast to remove air
Draw injectate
e.g., 80 mg methylprednisolone/0.5% bupivacaine, total volume 2 mL
Procedure Steps
Ensure correct spine level for injection
Angle equipment to maximize visualization of facet joint
Target lower 1/3 of joint space
Often, arthritic joints will have redundancy inferiorly, creating a more accessible joint space
Mark skin
Perform sterile prep and drape
Apply local anesthetic
Confirming trajectory of anesthetic needle may aid placement of spinal needle
Place spinal needle into subcutaneous tissue, and confirm trajectory with imaging
Advance until bone is reached or feel needle advance into joint space
If reach bone, “walk” needle into joint
Attach preloaded contrast tubing and syringe
Slowly inject only enough contrast to confirm needle tip in joint space
Document needle placement with imaging
Remix and attach injectate syringe
Slowly inject
May require high pressure injection via 1-3 mL syringe
Note patient’s symptoms during and immediately following injection
Remove needle, and attain hemostasis
Cleanse skin with hydrogen peroxide
Dry skin, and apply bandage
Synovial cyst therapeutic rupture
Same steps as FJI
Alternate approach is interlaminar puncture of cyst
CT guidance suggested for translaminar approach
Patient will often feel “pop” with cyst rupture
May require significant injection pressure
Can be quite painful for patient
Interventionalist will see sudden spread of contrast into epidural space with cyst rupture
Findings and Reporting
Document level of injection
Pain scale and pain characteristics
Before procedure
During injection
After procedure
Other symptoms/complications
Alternative Procedures/Therapies
Radiologic
Medial branch block
Epidural steroid injection
Percutaneous facet joint fusion
Surgical
Fusion
Other
Rhizotomy
Radiofrequency ablation
POST-PROCEDURE
Expected Outcome
Improved pain symptoms
Things to Do
Help patient from procedure table
Establish follow-up
Remind patient to keep pain diary until next clinic appointment
Things to Avoid
Strenuous activity for remainder of day
Bathing for 48 hours
OUTCOMES
Problems
Failure to alleviate pain
Technical failure
Wrong level injected
Injection extraarticular
Clinical failure
Facet joint not source of pain
May require multilevel injections
Multifactorial pain
Complications
Most feared complication(s)
Thecal sac puncture
Cord injury
Meningitis
Cerebrospinal fluid leak
Other complications
Bleeding
Infection
Nerve injury
SELECTED REFERENCES
1. Datta S et al: Systematic assessment of diagnostic accuracy and therapeutic utility of lumbar facet joint interventions. Pain Physician. 12(2):437-60, 2009
2. Martha JF et al: Outcome of percutaneous rupture of lumbar synovial cysts: a case series of 101 patients. Spine J. 9(11):899-904, 2009
Image Gallery
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


