FACIAL NERVE: DEVELOPMENTAL CONDITIONS
KEY POINTS
- Peripheral facial nerve palsy that presents in infancy or in a younger patient may be of developmental origin.
- Peripheral facial nerve palsy that presents as slow or stuttering in onset, is recurrent, or does not recover requires very detailed magnetic resonance and computed tomography studies of the facial nerve to search for a structural lesion that is very likely to be present in those atypical settings for Bell palsy.
- Atypical presentations of peripheral facial nerve palsy may be due to specifically treatable infectious and noninfectious inflammatory diseases even when a congenital cause is suspected.
- Imaging can be very helpful to triage patients with peripheral facial nerve palsy to the next best step in the diagnostic process.
In general, developmental abnormalities related to the facial nerve present during childhood. Some manifest in infancy; however, the presentation is often delayed until sometime beyond infancy and well into the early adult years, even into middle age. If they grow, the growth tends to be at the same rate of normal structures, including a rapid phase at times of accelerated growth of the individual—for instance, in adolescence. Some, such as high-flow vascular malformations, have internal physiologic dynamics that will allow them to enlarge more rapidly than normal tissues rather than truly proliferate. Truly neoplastic developmental conditions such as teratomas or proliferative hemangiomas (Chapters 8 and 9) will manifest growth out of proportion to normal structures.
Developmental abnormalities related to the facial nerve are only infrequently discovered incidentally (without facial nerve symptoms and signs) on imaging studies done for purposes other than hearing loss or aural atresia. Facial nerve developmental conditions may present as a mass, for instance, in the parotid or retrotympanic region. Such masses may range from a congenital cholesteatoma (Fig. 128.1) to a plexiform neurofibroma. More commonly, they will cause facial weakness or hemifacial spasms in the absence of a mass that can be detected by physical examination. Epineural cysts are uncommon, possibly congenital abnormalities that might explain facial nerve motor dysfunction (Fig. 128.2A–F). Other anatomic variants, arachnoid cysts, and arachnoid granulations occur, but their relationship to facial nerve symptoms such as weakness and especially hemifacial spasm remains speculative (Fig. 128.2G–I).
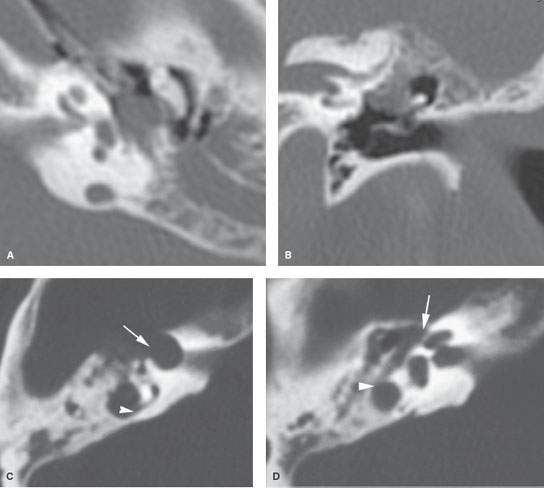
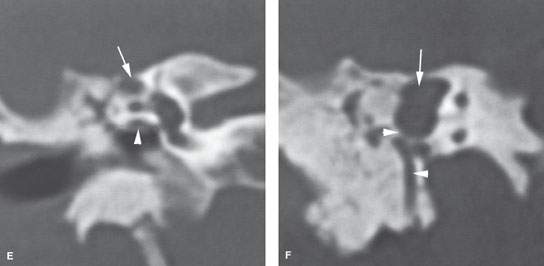
FIGURE 128.1. Imaging findings in congenital cholesteatoma affecting the facial nerve in two patients. A, B: Patient 1 has a nodular soft tissue mass, located medial to the ossicles, growing along the tympanic segment of the facial nerve and associated with anomalous temporal bone development. C–F: Patient 2 has a well-demarcated soft tissue mass, expanding and eroding the surrounding bone as seen on computed tomography. In (C), the cholesteatoma involves the anterior genu of the facial nerve (arrow) and extends posteriorly to erode the bone over the superior semicircular canal (arrowhead). In (D), the cholesteatoma (arrow) is near but does not involve the second genu (arrowhead). In (E), the coronal image shows that the cholesteatoma is above the lateral semicircular canal (arrow); thus, a nerve sheath tumor is very unlikely given the normal bony tympanic segment canal (arrowhead). In (F), the coronal section more posteriorly further confirms that the cholesteatoma (arrow) is separate from the second genus and descending facial canal (arrowhead). (NOTE: A facial nerve tumor was suspect because the original interpreter did not properly consider the anatomy of the facial canal relative to the compressing but entirely extrinsic congenital cholesteatoma. A congenital cholesteatoma was found at surgery.)
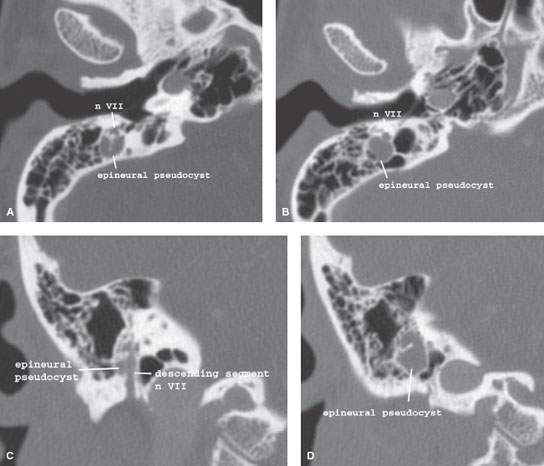
FIGURE 128.2. Three patients with “cysts” along the course of the facial nerve. A–D: Patient 1 with epineural pseudocysts of the facial nerve canal and hemifacial spasms. A round, well-demarcated cystic lesion could be an isolated, enlarged mastoid air cell or epineural cyst as proven pathologically abutting the mastoid segment of the facial nerve. E, F: Patient 2 with epineural pseudocysts of the facial nerve canal and hemifacial spasms. A round, well-demarcated pathologically proven epineural cyst (arrow) eroding the mastoid segment of the facial nerve (arrowheads). G–I: Patient 3. A cystic zone surrounds the first genu of the facial nerve (arrows) compared to the more normal first genu on the right (arrowhead in G).
The more common asymptomatic congenital abnormalities of the facial nerve are those related to an aberrant course as isolated findings; anatomic variations are discussed in Chapter 104 (Fig. 104.54). They are also commonly seen in patients with obvious aural atresia or in those who have a conductive hearing loss but otherwise occult maldevelopment of the stapes, oval window region, and facial nerve in concert. Those conditions, dealing specifically with temporal bone abnormalities, are described in Chapters 105 and 106 (Figs. 105.8, 105.15, 106.6, and 106.13). Syndromic associations were introduced in Chapter 107. Hypoplasia or aplasia of the facial nerve can be seen in isolation or as part of Moebius syndrome (Figs. 128.3 and 128.4).
The natural history and imaging appearance of the other somewhat uncommon developmental abnormalities that affect the facial nerve are discussed in dedicated chapters on those topics, including epidermoid and dermoid cysts and related abnormalities (Chapters 8 and 134), vascular abnormalities (Chapters 9 and 132), and facial nerve abnormalities in association with a persistent stapedial artery (Chapter 108).
This chapter will discuss congenital cholesteatoma, perineural cystic lesions that may be of congenital origin and affect the facial nerve, and Moebius syndrome. This and the other chapters just described should constitute a reasonably complete description of developmental conditions that may affect the facial nerve and that are likely to be encountered in an imaging practice.
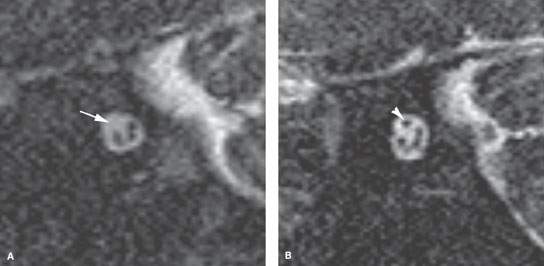
FIGURE 128.3. Congenital aplasia of the facial nerve. In a newborn with unilateral facial nerve palsy, isolated facial nerve aplasia is seen as a missing facial nerve on parasagittal three-dimensional steady state images (arrow in A). The other internal auditory canal shows the normal four nerves present; facial nerve is, located anteriorly and superiorly in the canal (arrowhead in B).
ANATOMIC AND DEVELOPMENTAL CONSIDERATIONS
Embryology
The development of the facial nerve within the temporal bone is intimately linked to that of the middle and inner ear, as discussed in Chapters 105 and 106, since the primordia of the facial and cochleovestibular nerves begin in very close proximity at the beginning of gestation. The development of the nerves will then be affected by that of the otic capsule and maturation of the first and second branchial arches as the latter relate to the development of temporal bone and the face, especially the mandible. More proximally, disorders of rhombencephalic development can lead to absence or hypoplasia of the facial nerve, usually in association with other cranial nerve absence or hypoplasia, craniofacial anomalies, and other genetic anomalies.
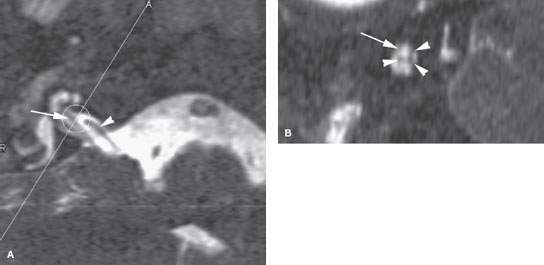
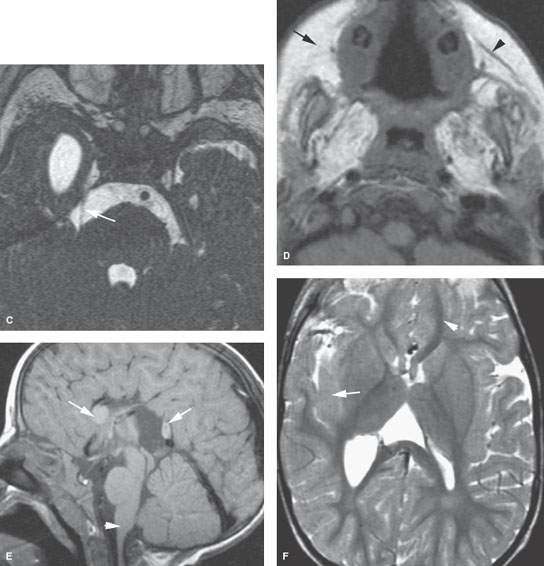
FIGURE 128.4. Unusual variant of Moebius syndrome. A: Three-dimensional steady state image showing the typically normal cochlear nerve (arrow) and a vascular loop (arrowhead). Line A shows the plane of the oblique sagittal reformation in (B). B: Three-dimensional steady state image showing the absent facial nerve (arrow) with the divisions of cranial nerve VIII (arrowheads). C: Three-dimensional steady state image showing a very small trigeminal nerve (arrow). D: T1-weighted image showing the lack of development or atrophy of the muscles of facial expression more on the right (arrow) than the left (arrowhead) and almost absence of the muscles of mastication. E: Malformations of the corpus callosum (arrows) and brain stem (arrowheads). F: T2-weighted image showing gray matter migrational abnormalities (arrow).
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


