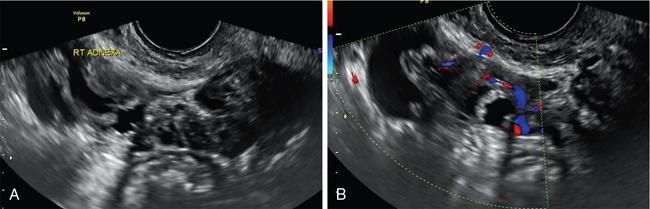
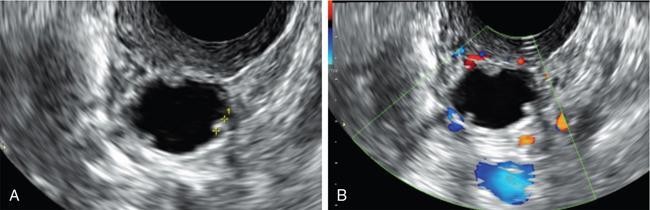
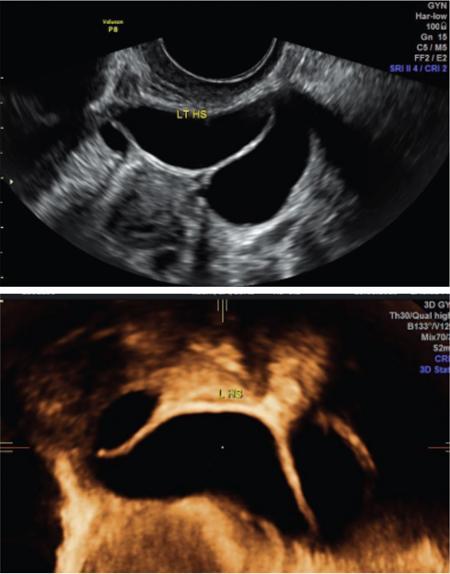
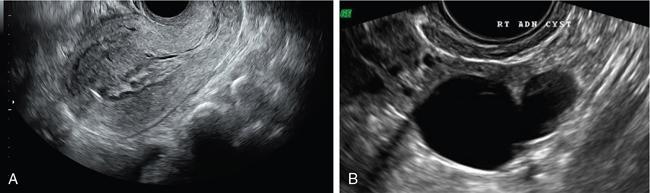
John De Lindsay, Subhashree C SALPINGITIS Salpingitis refers to the diffuse inflammation of the fallopian tubes and can be unilateral or bilateral. It is the most common early form of PID. Salpingitis has the highest risk of infertility and ectopic pregnancies. Coexisting endometritis can be seen in up to 70%–90% of nonobstetric patients. The clinical presentation in salpingitis can be variable, from being asymptomatic to severe pelvic discomfort and tenderness. Poor correlation is often noted between the degree of symptoms and the extent of tubal inflammation. In salpingitis, the fallopian tubes become hyperemic and swollen due to inflammation. With suppurative salpingitis, the lumen of the tube distends with pus and spills over into the peritoneal cavity, coating the serosa of the adjacent uterus and ovary. US maybe used as the first-line imaging modality for evaluating suspected salpingitis. Subtle abnormalities such as fallopian tubal tenderness with tortuosity, increased wall vascularity and tubal thickening of more than 5 mm may be considered pointers towards salpingitis. Salpingitis may be considered on CT when the fallopian tube thickening is more than 5 mm in axial dimension with enhancing walls (Fig. 11.17.1.1). Adjacent peritubal free fluid or cul-de-sac fluid may be other indicators. Fallopian tube thickening is the most specific sign to arrive at a diagnosis of salpingitis (Fig. 11.17.1.1). Chronic salpingitis may present as diffuse tubal irregularity with narrowing or complete obliteration of the tubes. Salpingitis isthmica nodosa is a benign inflammatory process causing nodular scarring of the fallopian tubes. At hysterosalpingography, tubal irregularity and subcentimetric protrusions from the isthmic portion of the tube are seen. PELVIC INFLAMMATORY DISEASE Pelvic infection is one of the most frequent cause of pelvic pain in females. Diagnosis of pelvic inflammatory disease (PID) can be challenging because it mimics other abdominal and pelvic processes. Pelvic ultrasonography is the first line investigation of choice. Multimodality imaging with CT and MRI are required for making a definitive diagnosis and for assessing the extent of disease and complications. PID is a spectrum of disease where microorganisms cause an inflammatory continuum ascending from the lower genital tract to infect the uterus, fallopian tubes, ovaries and may extend to the peritoneal cavity. The infection begins with cervicitis and progresses to endometritis, salpingitis, pyosalpinx, tubo-ovarian complex and ultimately tubo-ovarian abscess (TOA) (Fig. 11.17.2.1). One-third to one-half of cases are due to chlamydia trachomatis or Neisseria gonorrhoeae. However, PID is most commonly (30%–40%) a polymicrobial infection and substantial proportion of cases are nongonococcal and nonchlamydial in origin. It may be due to vaginal flora, anaerobic gram-negative rods and Mycoplasma bacteria. Tuberculosis and actinomycosis occur less frequently. Risk factors for PID include young age, multiple sexual partners, an increased frequency of coitus and the presence of intrauterine contraceptive device. Secondary infection of adnexa from gastrointestinal origin like appendicitis and diverticulitis is also common. Clinical diagnosis of acute PID often presents a challenge due to overlap of symptoms and signs with conditions like endometriosis, appendicitis and ectopic pregnancy. Symptoms: Pelvic pain is the most common symptom, although may be absent or mild in some patients. Mucopurulent vaginal discharge and fever are the other usual symptoms. Signs: Per vaginal examination reveals cervical motion tenderness, uterine and adnexal tenderness. Chronic PID symptoms: Patients may be asymptomatic. They can present with chronic pelvic pain, low back ache, dyspareunia, abnormal vaginal bleeding and vaginal discharge. WBCs on saline microscopy of vaginal secretions, elevated ESR, CRP and leucocytosis. A delay in treatment of PID causes significant reproductive and gynaecologic morbidity, such as infertility, increased risk of ectopic pregnancy, chronic pelvic pain and recurrent infection. Hence there is need for proper and adequate treatment of this condition. Most patients can be treated as out-patients with broad spectrum antibiotics. Hospitalisation is required in severe cases like TOA (Fig. 11.17.2.2). Inflammation of uterine cervix. May be infectious or noninfectious. Infectious cervicitis represents early presentation of PID. USG shows an enlarged cervix and hyperaemic cervical canal. CT and MRI show an enhancing endocervical canal. Cysts can be seen lining the endocervical canal. Cervical stroma is usually intact. Differentiation from cervical malignancy is made by lack of enhancing solid components in the abnormal cervix. Inflammation of the endometrial lining of uterus. Usually occurs during pregnancy or postpartum state or gynaecologic instrumentation. USG imaging findings depend on stage of PID. In early or mild infection, the findings are nonspecific. Endometritis may not exhibit any sonographic findings. A fluid-filled endometrial cavity is suggestive of endometritis in the setting of fever, vaginal discharge and uterine tenderness on physical examination. Intrauterine fluid is a nonspecific finding. Gas in the endometrial cavity will appear as foci of increased echogenicity with posterior dirty shadowing. Presence of gas increases the possibility of infection, though gas in the endometrial cavity can be present postpartum and postinstrumentation. Fluid in cul-de-sac is again a nonspecific finding. Internal echoes within the fluid could suggest infection (or haemorrhage) (Fig. 11.17.2.3A).
11.17: Fallopian tubes
Introduction
Clinical features
Pathology
Ultrasound
CT
Hysterosalpingogram
Introduction
Definition
Aetiology
Clinical features
Laboratory findings
Early stages of PID
Cervicitis
Endometritis
Definition
USG
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


