Imaging plays a critical role in the preoperative and postoperative evaluation of patients with femoroacetabular impingement. Non-contrast MR imaging and direct magnetic resonance arthrography of the hip are the modalities of choice for the preoperative assessment of chondrolabral lesions. The MRI protocol should include radial images for detailed analysis of the cam deformity and fast sequences covering the pelvis and knee for measurement of femoral torsion. In patients with postoperative pain, a comprehensive analysis of residual deformities and signs of osseous overcorrection should be performed as they can cause residual impingement or iatrogenic instability.
Key points
- •
Biplanar radiographs are the basis of the diagnostic workup in femoroacetabular impingement (FAI).
- •
MR imaging of the hip should include radial images for evaluation of cam deformities and sequences of the pelvis and condyles for assessment of femoral torsion.
- •
Femoral torsion can be reliably measured on MR imaging but differs considerably based on the used measurement method.
- •
Status of joint degeneration can help predicting outcome of FAI surgery.
- •
Residual osseous deformities are the most common reason for recurrent pain after FAI surgery and should be looked for on postoperative hip MR imaging.
Introduction
The definition of femoroacetabular impingement (FAI) as a pathomechanic concept in the early 2000s, along with advances in surgical techniques, has led to an exponential increase in the number of joint-preserving procedures performed worldwide. In FAI, osseous deformities of the proximal femur and/or acetabulum impair the normal physiologic range of motion and create a repetitive mechanical conflict. Over time, this leads to damage to the acetabular cartilage and labrum which causes pain and can cause early osteoarthritis of the hip. Arthroscopic or open surgery for FAI aims to correct the underlying osseous deformities; thereby, improving biomechanics and range of motion, reduce pain, and ideally preserve the native hip joint in the long term.
Imaging plays a pivotal role in preoperative and postoperative assessment of FAI. Conventional biplanar radiographs remain the basis of the diagnostic pyramid allowing an initial patient stratification, as patients with substantial damage to the hip joint do not benefit from a joint-preserving procedure. In addition, radiographs are used to assess acetabular coverage and screen for cam deformities. , In patients with FAI syndrome, MR imaging is then performed to assess chondro-labral lesions. In addition, MR imaging is used to obtain a detailed assessment of the morphology of the femoral head neck junction and assess femoral torsion. In patients with postoperative pain, a detailed assessment of hip MR imaging is warranted with knowledge of normal postoperative appearance and the common complications related to FAI surgery. , This article discusses the current MR imaging standard in preoperative planning and postoperative evaluation of FAI.
Cam femoroacetabular impingemt
Pathomechanism and Surgical Treatment of Cam Femoroacetabular Impingement
In primary cam FAI, an aspherical extension of the femoral epiphysis which arises during the adolescent growth spurt creates an osseous asphericity which repetitively abuts against the anterior acetabular rim. During hip flexion and internal rotation, the excess bone moves into the joint cavity inducing initial separation to the chondro-labral junction which progresses to cartilage delamination and detachment of the labrum from its base. Femoral osteochondroplasty is performed with the goal of restoring the sphericity of the femoral head-neck junction.
Imaging of Cam Femoroacetabular Impingement
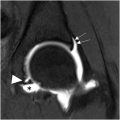
While anteroposterior (AP) pelvis views demonstrate the superiorly located pistol grip deformity, lateral views such as the modified Dunn view better demonstrate anterior located cam deformities. However, radiographs alone cannot rule out the presence of a cam deformity as they fail to visualize the entire circumference of the proximal femur. Radial images which use the femoral neck as axis of rotation are considered the gold standard for assessment of the cam deformity. Due to the fact that cam deformities are usually most pronounced at the anterosuperior femoral neck, the radial images are also more sensitive than oblique axial images which are aligned with the femoral neck. Accordingly, radial images are commonly recommended in the preoperative workup of FAI. These images can be either acquired as 2-dimensional (2D) turbo/fast spin echo sequences or are reformatted from a 3-dimensional (3D) gradient echo sequence. On these images, the extension of the cam deformity can be precisely assessed topographically using the most prominent appearance of the greater trochanter as reference for the superior 12 o’clock position, with 3/9 o’clock position reflecting anterior and posterior, respectively ( Fig. 1 ). Knowledge of the asphericity location is crucial, as resection of posterior cam lesions poses technical challenges due to proximity to superior retinacular vessels which maintain the blood supply to the femoral head. Despite frequent usage in research settings, alpha angle measurement (alpha angle >60° consistent with a cam deformity) is not recommended due to inherent measurement error. Instead, a descriptive report detailing cam deformity extension and severity is advocated.

Imaging of pincer femoroacetabular impingement
Pathomechanism and Surgical Treatment of Pincer Femoroacetabular Impingement
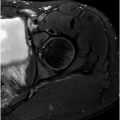
Pincer deformities encompass a continuum of varying degrees of acetabular overcoverage and acetabular retroversion. Unlike cam FAI, the femoral head does not protrude into the joint cavity but impacts against a too prominent and/or maloriented acetabular rim. This results in more circumferential narrow strips of cartilage damage and degeneration of the labrum substance with ossification and hypotrophy. Surgical treatment aims to restore normal range of motion without sacrificing too much weight-bearing cartilage surface by trimming of the acetabulum followed by labrum refixation. This is especially important when it comes to severe acetabular retroversion which reflects a malrotation of a normal-sized cup rather than actual overcoverage ( Fig. 2 ). Selected patients without severe joint damage benefit more from an anteverting periacetabular osteotomy than acetabular rim trimming as it normalizes the orientation of the acetabulum without reducing the joint contact area (see Fig. 2 ).

Imaging of Pincer Femoroacetabular Impingement
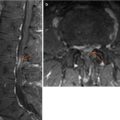
AP pelvis radiographs still remain the most important modality when it comes to assessment of acetabular coverage which is commonly performed with the lateral center edge angle and the acetabular index. These measurements reflect lateral acetabular coverage and inclination of the acetabulum, respectively. Physiologically, the acetabulum is anteverted which reflects an anterior opening of the acetabular cup and medial projection of the anterior acetabular wall relative to the posterior wall on radiographs and increases from cranially to caudally. Acetabular retroversion reflects a posterior opening of the acetabular cup and can be either limited to the superior acetabular rim or reflect a more global rotational deformity. Acetabular retroversion is assessed using the radiographic cross-over, posterior wall, and ischial spine signs , (see Fig. 2 ). However, radiographs only reflect a 2D representation of a complex 3D anatomy and are affected by pelvic tilt and rotation and changes between standing and supine image acquisition. By contrast, recent convolutional neuronal networks can be used to render fully-automated 3D MR imaging models of the acetabulum and cartilage layers. These models may be further used for quantitative morphologic analysis to potentially improve the characterization of abnormal acetabular coverage and version ( Fig. 3 ).

Femoral Torsional Deformities Pathomechanism and Surgical Treatment of Femoral Torsional Deformities
Femoral torsion refers to the sagittal orientation of the proximal femur relative to the distal femoral condyles. Femoral torsion strongly affects the impingement-free range of motion of the hip joint. Physiologically, normal femoral antetorsion ensures a balanced range of hip internal/external rotation. , Decreased femoral torsion (“retrotorsion”) decreases the range of hip internal rotation, predisposes to anterior impingement, and can further aggravate impingement due to classic FAI deformities. Conversely, excessively increased femoral antetorsion decreases the range of hip external rotation. Thereby, it can compensate an anterior impingement conflict but also lead to posterior ischiofemoral impingement. This extra-articular impingement conflict occurs between the posterior intertrochanteric region/lesser trochanter and the ischial tuberosity. Anterior leverage of the femoral head can cause secondary overload to the anterior acetabulum rim. To date, the indication for concomitant femoral derotational osteotomies to correct torsional deformities is still debated. However, there is common consensus that assessment of femoral torsion should be routinely performed in every patient eligible for joint-preserving hip surgery.
Measurement of Femoral Torsion
Since radiographs and clinical assessment are not reliable for assessment of femoral torsion, computed tomography (CT) has historically been considered as gold standard modality for torsional analysis. More recently, MR imaging-based measurements have been introduced as modality of choice. Using fast, consecutive, low-resolution sequences covering the pelvis including the proximal femur and the distal femoral condyles, the images can be acquired within 1 to 2 minutes without the need to change coils and patient positioning. MR imaging reportedly yields comparable accuracy as CT-based measurements of femoral torsion. While the bias between MR imaging and CT is within the measurement error and thus not clinically relevant, mean differences introduced by different measurement methods can be as high as 19° , ( Fig. 4 ). Notably, almost a dozen of different femoral torsion measurement methods have been described. These methods are based on different anatomic landmarks to define the proximal femoral reference line. They range from the level of the greater trochanter down to the lesser trochanter. , In general, femoral torsion angles increase when a more distal anatomic landmark is chosen to define the proximal femoral reference line. , In most centers, measurements are either performed at the level of the femoral neck axis (“Reikeras method” ) or distally at the level of the lesser trochanter (“Murphy method” ). Due to these differences, normal values depend on the applied measurement. To date, there is not sufficient data to clearly favor one measurement method over another, but for trigonometric reasons strictly axial slices over the proximal and distal femur should be acquired. , To prevent misdiagnosis related to different measurement methods, an institutional interdisciplinary standard should be established.

Ischiofemoral Impingement
In patients with ischiofemoral impingement due to excessively high femoral torsion, narrowing of the ischiofemoral space as well as quadratus femoris muscle edema have been reported as secondary diagnostic signs ( Fig. 5 A ). Absolute measurements of narrowing between the lesser trochanter and the ischial tuberosity are subject to alterations in hip rotation and are thus not sufficient as sole diagnostic criterion. Furthermore, clinical diagnosis of posterior extra-articular impingement is challenging. Thus, efforts have been made to improve the preoperative assessment of ischiofemoral impingement. Deep learning-based automated rendering of 3D MR imaging followed by virtual impingement testing using collision detection software has shown utility in improving diagnosis of extra-articular hip impingement ( Fig. 5 B).

Intra-articular lesions
Labrum Lesions
Surgical repair of a torn labrum is warranted whenever possible to restore its sealing function which maintains an even peak stress distribution and ensures joint stability by increasing the joint contact surface area. , Labrum repair in patients undergoing FAI surgery yields excellent long-term results. Accordingly, assessment of chondro-labral damage on hip MR imaging is of great importance. Depending on institutional preference, non-contrast MR imaging of the hip or direct MR-arthrography is performed. This includes a protocol with unilateral high-resolution images in coronal, sagittal, axial-oblique, and radial orientation. Fast-/turbo-spin echo images with either T1-w and/or PD-w images are routinely acquired. A detailed assessment of the acetabular labrum should include description of tear location, labrum size, and tear pattern. , This can inform surgical planning, for example, in cases of severe degenerative labrum tearing in pincer FAI requiring labrum reconstruction. In addition, labrum hypertrophy and mucoid degeneration may indicate a compensatory adaption to hip instability secondary to hip dysplasia or excessively high femoral torsion , ( Fig. 6 ). Thus, a detailed assessment of labrum morphology may aid surgeons as they contemplate when to perform isolated FAI correction or to perform an additional pelvic-/femoral osteotomy. This is important in patients with combined deformities such as patients with a cam deformity and associated borderline dysplasia (lateral center edge angle 20°–25°).