Fig. 33.1
Heart exposure and ligation of second diagonal artery
We hypothesize that fluorescein will provide a detailed anatomic demarcation of the ischemic myocardium and help us document tissue recovery after reperfusion. Considering that direct visualization of the injured myocardium does not allow clear identification of the compromised area, we believe that our study has a potential clinical application.
Although multiple authors have studied ischemia-induced cardiac injury in animal models, to our knowledge this is the first study demonstrating an in-vivo method for direct visualization of the injured myocardium [2].
Materials and Methods
All animal protocols were approved by the Institutional Animal Care and Use Committee (IACUC) at University of Buenos Aires. All studies were performed at Hospital de Clinicas “Jose de San Martin.”
Fluorescein
Fluorescein is an organic compound, slightly soluble in water and alcohol. It is a fluorophore widely utilized as diagnostic tool in the field of ophthalmology and optometry. It has also been shown to be appropriate to evaluate hepatic function and liver blood flow. Originally described by Dr. Johann Fiedrich Wilhelm Adolf Baeyer (1835–1917) who was awarded with the Nobel Prize in biochemistry for his discovery. The fluorescence of this molecule is very intense; peak excitation occurs at 494 nm and peak emission at 521 nm (Fig. 33.2). Fluorescein has been used safely in humans in the past, but some side effects including nausea, vomiting, hives, hypotension, and rarely anaphylactic shock have been described in the past.
Fig. 33.2
Fluorescein spectrum
Ten New Zeeland (N = 10) rabbits were used for this study. Each rabbit served as its own control. General anesthesia was achieved using 35 mg/kg of ketamine in combination with 5 mg/kg of intramuscular xilacaine. The rabbits were clipped at the sternal and ear level. Intravenous access was achieved by placement of a 20-gauge angiocath in the area of the left pinna. A lateral tracheostomy was placed using a number 3 endotracheal tube to secure the airway. Pediatric ventilators were used. Propofol and fentanyl were utilized to achieve proper sedation and analgesia.
The surgical technique included: sternotomy, pericardiectomy, cardiac luxation, and ligation of the second diagonal artery with 6.0 polypropylene suture (Fig. 33.1).
The ischemic area was analyzed under the xenon and UV light before and after the administration of 0.01 mg/kg of sodium fluorescein. Blood samples were taken and quantification of cardiac enzymes including CK, CK-MB, LDH, and Troponin was done before and 90 min after the induced ischemia. Oxygen saturation, heart rate, respiratory rate, and EKG were monitored continuously.
All the animals were euthanized according to the IACUC UBA regulations. The heart and lungs were resected en bloc, and submitted to the pathology department.
Results
Ten New Zeeland (N = 10) rabbits with a mean average body weight of 3.1 ± 0.6 kg were used for this study. No perioperative mortality was noticed and all the rabbits were euthanized at the end of the study.
Every rabbit functioned as its own control. Initial EKG, HR, RR, and oxygen saturation were measured and used as baseline (BL) values. No abnormalities were found on these parameters confirming an adequate health status of the animals.
No significant difference was observed between the values for pre- and post-myocardial infarction in the categories of heart rate (145 ± 5 bits/min) or respiratory rate (28 ± 5 breaths/min). Consistently, no variation was appreciated in the saturation of oxygen post myocardial infarction (97 ± 2 %).
On the contrary, an ST (1.8 ± 0.65 mm) elevation was observed in the EKG tracing immediately after the ligation of the second diagonal artery.
Biochemical (enzymatic) analysis was performed at baseline and at 90 min after complete occlusion of the second diagonal artery. These were compared using Student’s t test. Results were considered significant when the p value <0.05.
LDH (BL) 159.7 ± 112.2 (U/L) vs. LDH (PI) 1,012 ± 359.9 (U/L) (p < 0.0000781).
CPK (BL) 1,072 ± 121.7 (U/L) vs. CPK (PI) 359.5 ± 95.7 (U/L) (p < 0.00000002).
CPK-MB (BL) 0.89 ± 0.42 (ng/ml) vs. CPK-MB (PI) 3.89 ± 1.9 (ng/ml) (p < 0.00028593).
Troponin (BL) 0.06 ± 0.06 (ng/ml) vs. Troponin (PI) 19.6 ± 5.9 (ng/ml) (p < 0.00000005) (see Table 33.1).
Table 33.1
Results
Cardiac enzymes | Baseline | Post-ischemia | P value |
|---|---|---|---|
Troponin (ng/ml) | 0.06 ± 0.06 | 19.6 ± 5.9 | 0.00000005 |
CPK (U/L) | 1,072 ± 121.7 | 359.5 ± 95.7 | 0.00000002 |
CPK-MB (ng/ml) | 0.89 ± 0.42 | 3.89 ± 1.9 | 0.00028593 |
LDH (U/L) | 159.7 ± 112.2 | 1,012 ± 359.9 | 0.00000781 |
The infarcted area was analyzed with the xenon and UV light before and after the administration of fluorescein 0.01 ml/kg via peripheral intravenous injection. Prior to the administration of fluorescein, the xenon and UV light failed to delineate the compromise-ischemic area (see Fig. 33.1).
Despite the injection of fluorescein, the infarcted area was still not demarcated when the specimen was observed under the xenon light. However, a significant contrast was observed between the well vascularized tissue and the infarcted area when evaluated under UV light (see Figs. 33.3a–c and 33.4). The area measured 0.722 ± 0.39 cm2.
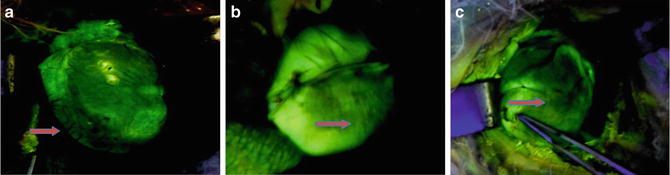
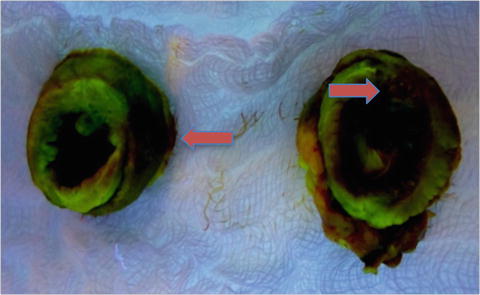
Fig. 33.3
Anterior (a), lateral (b) and inferior (c) view of the ischemic heart under UV light after the administration of fluorescein
Fig. 33.4
 Intraoperative Evaluation of Regional Portal Uptake Function
Intraoperative Evaluation of Regional Portal Uptake Function
 Application of Photodynamic Treatment
Application of Photodynamic Treatment
 Real-Time Assessment of Intestinal Perfusion by Fluorescence-Based Enhanced Reality
Real-Time Assessment of Intestinal Perfusion by Fluorescence-Based Enhanced Reality
 Detection of Bile Leakage After Hepatic Resection by Intraoperative Indocyanine Green Fluorescent Imaging
Detection of Bile Leakage After Hepatic Resection by Intraoperative Indocyanine Green Fluorescent Imaging
 Development of a Non-blurring, Dual-Imaging (X-Ray/Fluorescence) Tissue Marker for Localization of Gastrointestinal Tumors
Development of a Non-blurring, Dual-Imaging (X-Ray/Fluorescence) Tissue Marker for Localization of Gastrointestinal Tumors
 Fluorophore-Conjugated Chimeric Anti-CEA Antibodies for Fluorescence-Guided Surgery of Gastrointestinal (GI) Tumors
Fluorophore-Conjugated Chimeric Anti-CEA Antibodies for Fluorescence-Guided Surgery of Gastrointestinal (GI) Tumors




Transverse view of the heart after administration of fluorescein. Arrows indicate the ischemic area. Left image Area 1 and right image Area 2
Related posts:
Intraoperative Evaluation of Regional Portal Uptake Function
Application of Photodynamic Treatment
Real-Time Assessment of Intestinal Perfusion by Fluorescence-Based Enhanced Reality
Detection of Bile Leakage After Hepatic Resection by Intraoperative Indocyanine Green Fluorescent Imaging
Development of a Non-blurring, Dual-Imaging (X-Ray/Fluorescence) Tissue Marker for Localization of Gastrointestinal Tumors
Fluorophore-Conjugated Chimeric Anti-CEA Antibodies for Fluorescence-Guided Surgery of Gastrointestinal (GI) Tumors
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
