Foot(II)
Overview of Pediatric and Congenital Foot Deformities
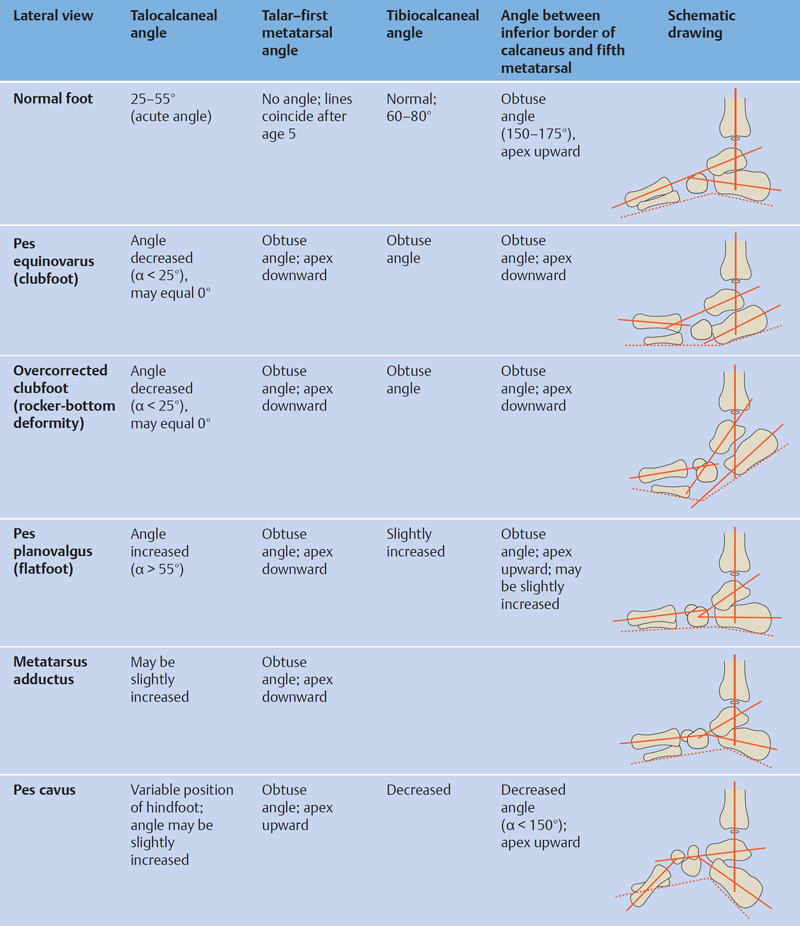
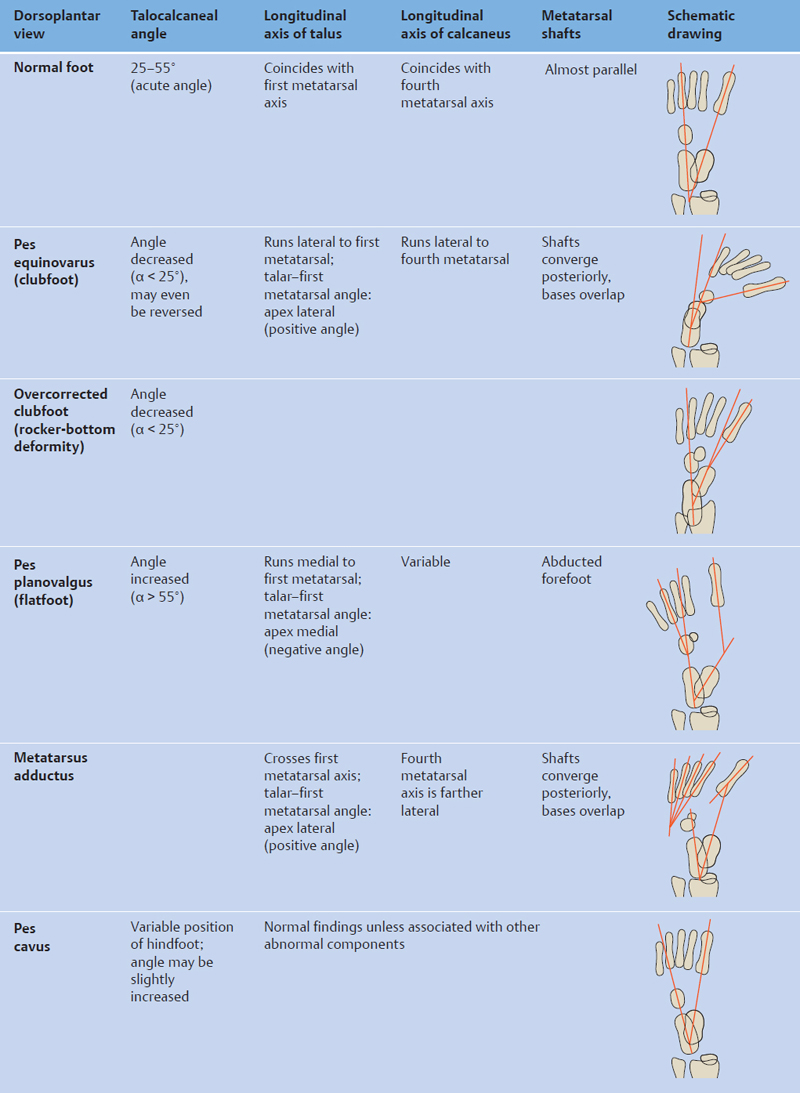
Descriptions of congenital and pediatric foot deformities vary widely in the literature, and varying techniques have been used in their radiographic measurement. Figs. 4.21 and 4.22 review the diagnostic work-up of pediatric foot deformities based on three studies conducted in patients 0–12 years of age. A common feature of all the studies is that the authors placed key emphasis on the evaluation of the hindfoot.
Specific deformities, measurements, and diagnostic techniques are described more fully in the sections below.
Davis LA, Hatt WS. Congenital abnormalities of the feet. Radiology 1955;64(6):818–825 Gamble FO, Yle I. Clinical Foot Roentgenology. 2nd ed. Huntington NY: Krieger Publishing; 1975 Ritchie GW, Keim HA. A radiographic analysis of major foot deformities. Can Med Assoc J 1964;91:840–844 Templeton AW, McAlister WH, Zim ID. Standardization of terminology and evaluation of osseous relationships in congenitally abnormal feet. Am J Roentgenol Radium Ther Nucl Med 1965;93:374–381Foot Deformities in Children and Adults
Flatfoot (Pes Planovalgus)
Because the components of flexible flatfoot deformity in children and adolescents are basically the same as in acquired flatfoot in adults (usually caused by tibialis posterior tendon dysfunction), radiographic examination and interpretation are identical. Flattening of the longitudinal pedal arch is typically accompanied by valgus deviation of the hindfoot and abduction of the forefoot ( Figs. 4.23 and 4.24 ).
The components of the deformity can be diagnosed and quantified on standard radiographs of the foot based on the parameters listed in Table 4.2 .
While the calcaneal inclination angle is used to evaluate the flattening of the longitudinal arch, the talar declination angle and talar–first metatarsal angle describe the inferomedial angulation of the talus. The talocalcaneal angles evaluate the valgus position of the hindfoot whereas the talar–first metatarsal angle (dorsoplantar view) quantifies the degree of forefoot abduction.
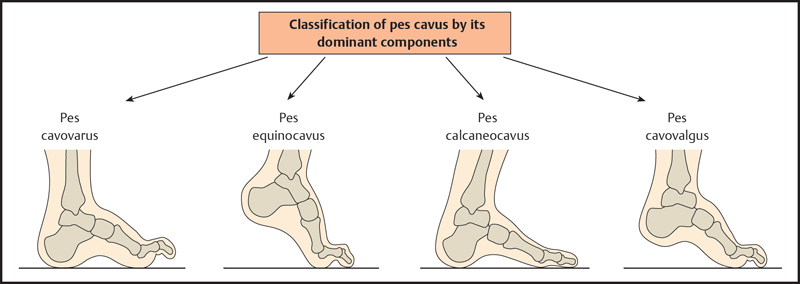
Pes Cavus
Pes cavus is a foot deformity in which the forefoot is fixed in plantar flexion, creating an abnormally high longitudinal arch. Subtypes are identified on the basis of clinical findings and the position of the hindfoot ( Figs. 4.25 and 4.26 ). If the dominant features are inclination of the forefoot and associated toe deformities, the condition is classified as pes cavovarus. Pes calcaneocavus is characterized by an increased vertical position of the heel. Measuring techniques can be used to evaluate the different components of the deformity ( Table 4.3 ).
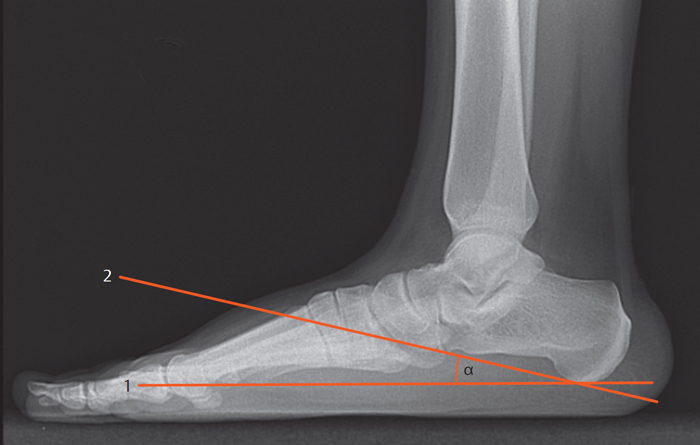
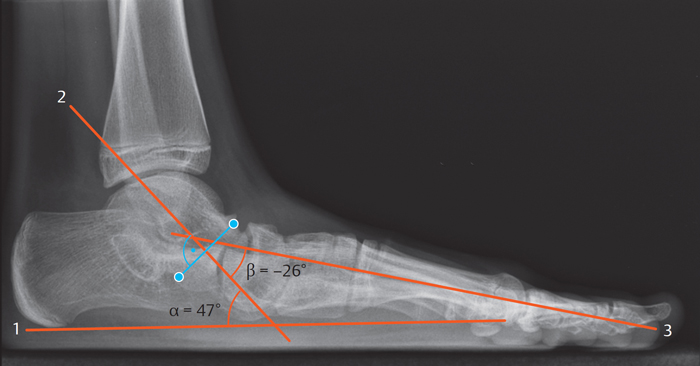
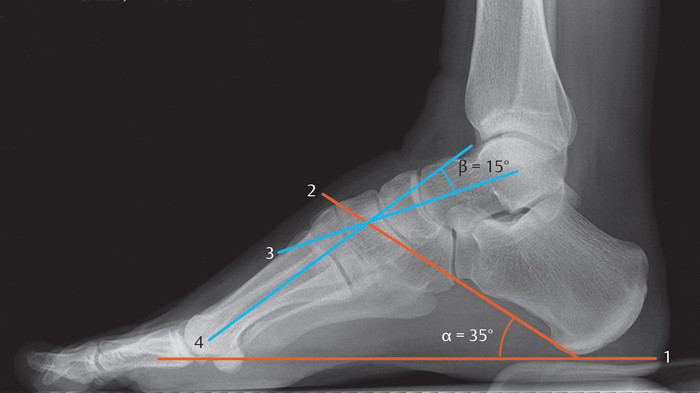
A vertical position of the calcaneus is the radiographic hallmark of pes calcaneocavus, in which markedly increased calcaneal inclination angles are typically found. The talar–first metatarsal angle is useful for quantifying the plantar flexion of the forefoot. Medial pes cavovarus is a relatively common form of pes cavus in which the inclination of the metastases decreases laterally to an almost normal alignment of the fifth metatarsal. The resulting crossed position of the first and fifth metatarsals is a characteristic feature of this deformity.
The position of the hindfoot is variable in pes cavus. In principle, the hindfoot may occupy a varus, neutral, or slightly valgus position. Varus is most common, however, and can be evaluated by measuring the talocalcaneal angles on dorsoplantar and lateral radiographs. Pes cavus is often accompanied by clawing of the lesser toes.
Metatarsus Adductus
Various terms have been used as synonyms for metatarsus adductus in the literature:
Pes adductus
Metatarsus varus
Forefoot varus
Sickle foot
The key feature of congenital metatarsus adductus is medial deviation of the forefoot at the level of the tarsometatarsal joints (Lisfranc joint). This differs somewhat from pes adductus, which is defined as a deviation the apex of which is located farther back at the level of the midtarsal joint (Chopart joint). In both deformities the hindfoot occupies a normal position or may be slightly everted.
As in other foot deformities, the radiographic analysis of metatarsus adductus is based on dorsoplantar and lateral radiographic views.
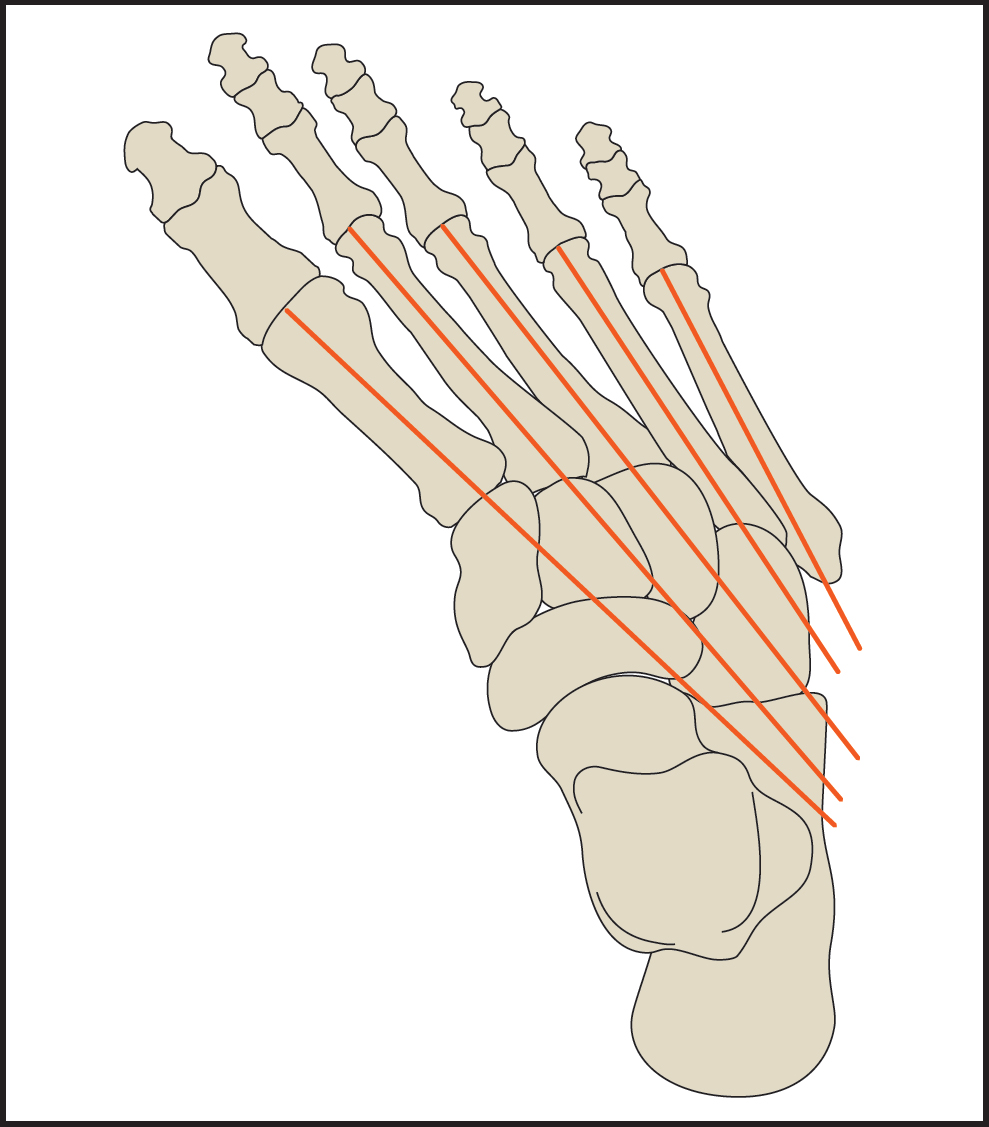
Metatarsal Convergence
The degree of medial deviation of the forefoot in metatarsus adductus decreases from the medial to lateral side. Viewed on a dorsoplantar radiograph of the foot, the longitudinal axes of the metatarsal shafts converge posteriorly and typically pass posterolateral to the tarsus. In a normal foot, the longitudinal axes of the metatarsals show only a slight degree of convergence and are directed posteriorly rather than posterolaterally ( Fig. 4.27 ).
Metatarsus Adductus Angle
The metatarsus adductus angle, measured on a dorsoplantar radiograph of the foot, describes the angle formed by the longitudinal axis of the lesser tarsus and the longitudinal axis of the second metatarsal ( Fig. 4.28 ). The metatarsals normally occupy a slightly adducted position relative to the lesser tarsus (10–20°). “Lesser tarsus” refers collectively to the cuneiform, cuboid and navicular bones.
As it is somewhat tedious to construct the longitudinal axis of the lesser tarsus, Engel recommends using the longitudinal axis of the medial cuneiform as an alternative. That line is roughly parallel to the longitudinal axis of the lesser tarsus.
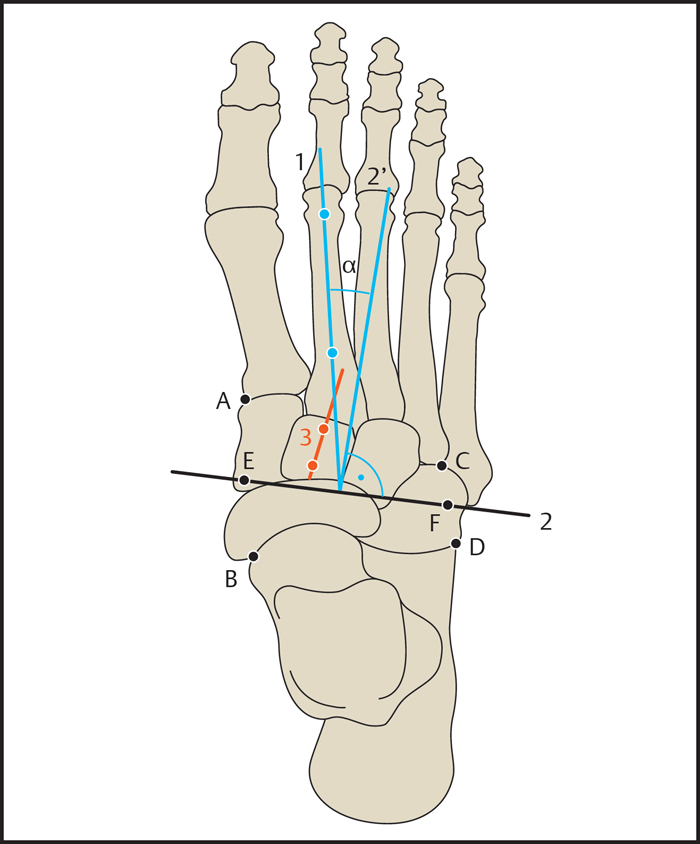
The precise longitudinal axis of the lesser tarsus is constructed as follows: First, two straight lines are drawn on the medial and lateral sides of the tarsus. On the lateral side, a line is drawn from the anterolateral corner of the calcaneus to the lateral proximal corner of the fourth metatarsal. On the medial side, a line is drawn through the medial corner of the talar articular surface of the talonavicular joint and through the medial proximal corner of the first metatarsal. The line connecting the midpoints of the medial and lateral lines is the transverse axis of the lesser tarsus. The longitudinal axis of the lesser tarsus is then found by drawing a line perpendicular to the transverse axis.
The longitudinal axis of the medial cuneiform deviates from that axis by ~ 3°. Ranges of normal values are listed below:
Metatarsus adductus angle
Metatarsus adductus angle:
Normal range: α = 10–20°
Metatarsus adductus: α > 20°
Simplified metatarsus adductus angle (Engel method):
Normal range: α = 13–23°
Metatarsus adductus: α > 23°
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


