Gastric Bezoar
Michael P. Federle, MD, FACR
Key Facts
Terminology
Intragastric mass composed of accumulated ingested (but not digested) material
Phytobezoar: Undigested vegetable matter
Trichobezoars: Accumulated, matted mass of hair
Lactobezoar: Undigested milk concretions
Pharmacobezoar: Bezoar comprised of medications
Imaging
Mobile intraluminal filling defect
Mottled appearance is result of air bubbles retained in interstices of mass
Small bezoars are rounded or ovoid
Tend to float on water-air surface surrounded by gastric contents
Pathology
High incidence of peptic ulcers, especially with more abrasive phytobezoars
Predisposing causes
Previous gastric surgery: Vagotomy, pyloroplasty, antrectomy, partial gastrectomy
Inadequate chewing, missing teeth, dentures
Overindulgence of foods with high fiber content
Altered gastric motility: Diabetes, mixed connective tissue disease, hypothyroidism
Clinical Issues
Bezoars usually form in stomach
May fragment and enter small bowel where they absorb water, increase in size, and become impacted
May present with small bowel obstruction
Endoscopic lavage fragmentation and extraction is safe and effective
Drinking several liters of cola beverage has been reported to clear all or portions of phytobezoars
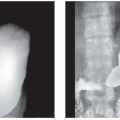
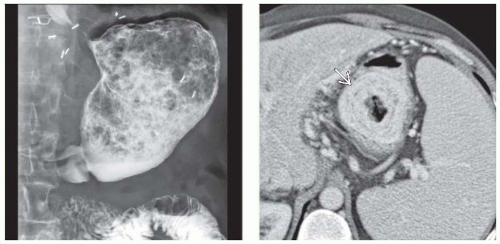 (Left) 60-year-old man with early satiety years after vagotomy and Billroth 1 surgery. Film from an upper GI series shows evidence of the prior surgery and a large heterogeneous “ball” of debris and gas within the stomach mixed with the barium. (Right) Axial CECT shows a laminated mass  in the stomach due to a phytobezoar. in the stomach due to a phytobezoar. |
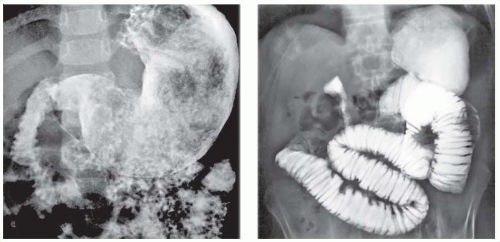 (Left) 3-year-old girl with vomiting. Upper GI series shows a fixed filling defect in the stomach with a swirled pattern of gas and solid material, found to represent a trichobezoar. (Right) Small bowel obstruction following a Billroth 2 procedure. Film from a small bowel follow through shows evidence of the prior gastric surgery and complete obstruction of antegrade flow of barium in the mid-jejunum. At surgery, a phytobezoar was removed, which corresponded to the shape and size of the gastric remnant. |
TERMINOLOGY
Definitions
Intragastric mass composed of accumulated ingested (but not digested) material
IMAGING
General Features
Best diagnostic clue
CT or fluoroscopy: Intraluminal mass containing mottled air pattern
Location
Sites of impaction: Stomach, jejunum, ileum
Narrowest portion of small bowel 50-75 cm from ileocecal valve or valve itself
Any part can be affected, especially in patients with postoperative adhesions
Morphology
Persistent concretions of foreign matter
Classified according to material composition
Phytobezoar: Undigested vegetable matter
Poorly digested fibers: Skin and seeds of fruits and vegetables
Diospyrobezoar: Persimmons
Trichobezoars: Accumulated, matted mass of hair
Trichophytobezoar: Both hair & vegetable matter
Lactobezoar: Undigested milk concretions
Pharmacobezoar: Bezoar comprised of medications
Radiographic Findings
Radiography
Abdominal plain film: Soft tissue mass floating in stomach at air-fluid interface
Mottled radiotransparencies in interstices of solid matter
± bowel obstruction
Insensitive test; bezoar identified in 10-18% of patients from radiographs alone
Fluoroscopic Findings
Intraluminal filling defect
With finely lobulated, villous-like surface
Freely mobile, without constant site of attachment to bowel wall
Barium or iodinated contrast media outline bezoar
Mottled or streaked appearance; contrast medium entering interstices of bezoar
Filling defect may occasionally appear completely smooth
Could be mistaken for enormous gas bubble that is freely movable within stomach
Coiled spring appearance (rare)
Partial or complete obstruction
Try to distinguish obstruction due to postoperative adhesions from bezoar-induced obstruction
CT Findings
Well-defined, oval, low-density, intraluminal mass
Mottled air pattern
Mottled appearance is result of air bubbles retained in interstices of mass
Heterogeneous mass without postcontrast enhancement
Pockets of gas, debris, fluid scattered throughoutRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree