Gastric Polyps
Michael P. Federle, MD, FACR
Key Facts
Imaging
Polyps classified into 3 types based on pathology
Hyperplastic, adenomatous, & hamartomatous
Hyperplastic polyps
Most common benign epithelial neoplasms of stomach (80-90%)
Virtually no malignant potential
Typical: Small, multiple, sessile (< 1 cm)
Location: Fundus & body
Fundic gland polyps: Now most common type
Associated with use of PPI medication
Adenomatous polyps
Less common (< 20% of benign polyps)
↑ risk of malignant change
Usually solitary, > 1 cm
Polyposis syndromes involving stomach
Familial adenomatous polyposis syndrome (FAPS)
Peutz-Jeghers syndrome
Top Differential Diagnoses
Retained food and pills
Gastric carcinoma (polypoid type)
Gastric metastases and lymphoma
Gastric GIST
Ectopic pancreatic tissue
Clinical Issues
Prevalence of gastric polyps in patients who have upper endoscopy = 6% (2009 study)
Fundic (77%), hyperplastic (17%), malignant (2%), adenomas (< 1%)
Much higher percentage of fundic polyps than in earlier studies
Caused by increased use of proton pump inhibitors medications
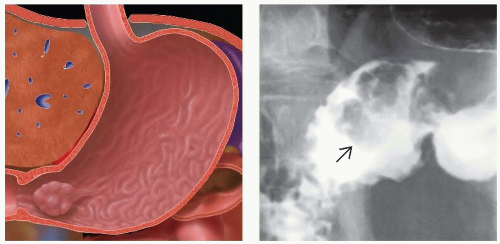 (Left) Graphic shows a pedunculated polyp in the gastric antrum, prone to prolapse through the pylorus with peristalsis. Any type of large polyp may prolapse in this fashion, including large hyperplastic, adenomatous, and even polypoid masses arising from the submucosa, such as lipomas. (Right) Upper GI series shows a polypoid mass  in the duodenal bulb that is a prolapsed gastric antral polyp (adenoma). in the duodenal bulb that is a prolapsed gastric antral polyp (adenoma). |
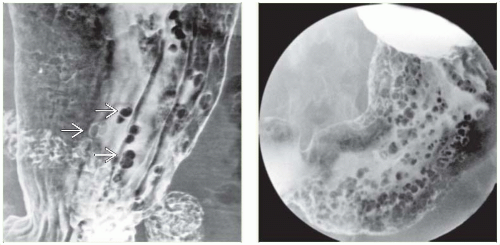 (Left) Film from an upper GI series in a 57-year-old man shows multiple small, sessile polyps  in the gastric body. The appearance and age of the patient are typical for hyperplastic polyps. (Right) Film from an upper GI series of adenomatous polyps in a patient with familial polyposis shows innumerable small polyps throughout the stomach. These are somewhat larger, more numerous, and more irregular in shape than most hyperplastic polyps. in the gastric body. The appearance and age of the patient are typical for hyperplastic polyps. (Right) Film from an upper GI series of adenomatous polyps in a patient with familial polyposis shows innumerable small polyps throughout the stomach. These are somewhat larger, more numerous, and more irregular in shape than most hyperplastic polyps. |
TERMINOLOGY
Definitions
Protruding, space-occupying, epithelial lesion within stomach
IMAGING
General Features
Best diagnostic clue
Radiolucent filling defect, ring shadow, or contour defect on barium study
Morphology
Hyperplastic polyps: Smooth, sessile, pedunculated
Fundic gland polyps: Always sessile, multiple, small
Adenomatous polyps: Usually single with lobulated or cauliflower-like surface
Hamartomas: Cluster of broad-based polyps
Other general features
85-90% of gastric neoplasms are benign
50% are mucosal and 50% submucosal
Gastric polyps are mucosal lesions
More common in hereditary polyposis syndromes
Polyps classified into 3 types based on pathology
Hyperplastic, adenomatous, & hamartomatous
Hyperplastic polyps
Most common benign epithelial neoplasms of stomach (80-90%)
Virtually no malignant potential
Typical: Small, multiple, sessile (< 1 cm)
Location: Fundus and body
Fundic gland polyps: Variant of hyperplastic polyps (< 1 cm)
Atypical large: Solitary, pedunculated (2-6 cm); location (body and antrum)
Atypical giant: Polyp (6-10 cm) multilobulated mass; location (antrum and body)
8-28% associated with atrophic gastritis, pernicious anemia, and cancer
Adenomatous polyps
Less common (< 20% of benign polyps); dysplastic lesions
↑ risk of malignant change via adenomacarcinoma sequence
Usually solitary, occasionally multiple, > 1 cm
Location: Mostly antrum > body
Histologically: Tubular (75%), tubulovillous (15%), villous (10%)
Gastric adenomatous polyps 30x less common than gastric cancer
Carcinoma in situ and invasive carcinoma: Seen in 50% of adenomatous polyps > 2 cm
30-40% associated with atrophic gastritis, pernicious anemia, and cancer
Higher risk of coexisting gastric cancer than risk of malignant change in polyp
Polyposis syndromes involving stomach
Familial adenomatous polyposis syndrome (FAPS)
> 50% of patients have gastric adenomatous polypsRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree