General Skeletal Patterns
GN5. Generalized Osteosclerosis
GN7. Soft-Tissue Calcification and Ossification
GN1 Acetabular Protrusion
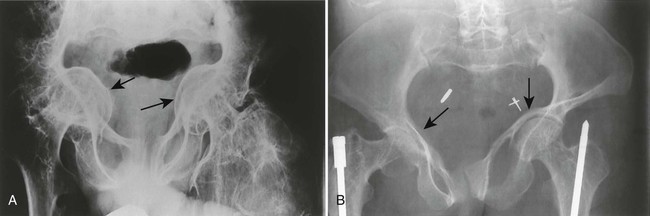
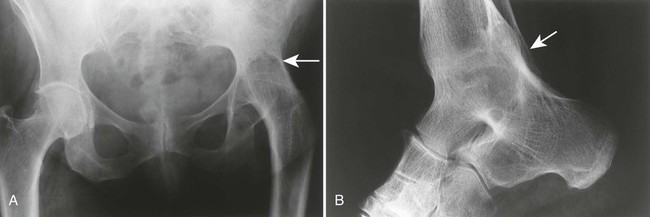
Protrusio acetabuli exists if, in a frontal projection of the pelvis, the dome of the acetabulum extends medially beyond a line segment drawn from the pelvic border of the ilium to the medial border of the body of the ischium (Köhler line). It is secondary to rheumatoid arthritis and Paget disease or may occur as a primary anomaly (Otto pelvis).
| Disease | Comments |
| Bone softening (Fig. 19-1) | Bone deformity resulting from congenital (osteogenesis imperfecta) or acquired bone-softening diseases (e.g., Paget disease, rickets, osteomalacia, osteoporosis) |
| Inflammatory arthritides | Most commonly associated with advanced rheumatoid arthritis of the hip; associated findings include osteopenia, uniform loss of joint space, bilateral distribution, nonproliferative joint margins; less commonly associated with rheumatoid variants (e.g., ankylosing spondylitis, psoriatic arthritis, Reiter syndrome, inflammatory bowel disease) |
| Miscellaneous disorders | Bone deformity resulting from posttraumatic remodeling, tumor, and infection |
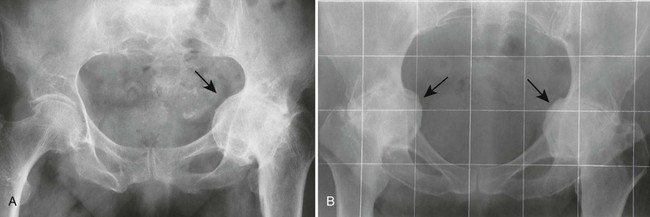
| Normal variant (Fig. 19-2) | May include medial protrusion of the femoral head in children |
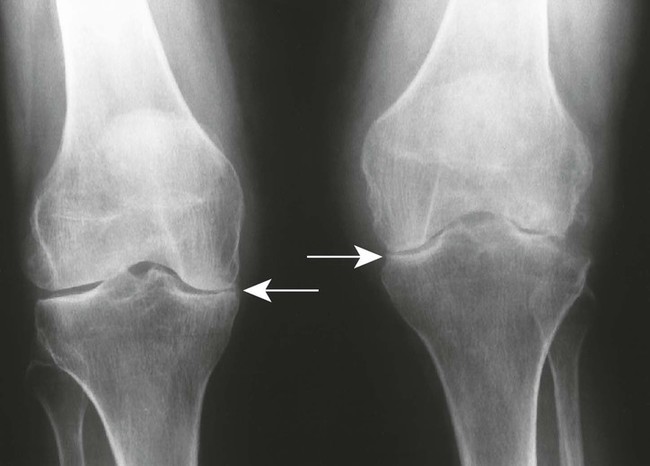
| Osteoarthritis (Fig. 19-3) (p. 544) | Usually less advanced degree of protrusion; patients manifest with a unilateral distribution of proliferative joint changes marked by nonuniform reduction of joint space; osteoarthrosis occurs secondary to trauma, hemophilia, ochronosis, and so on; in distinction to its listing here, osteoarthritis typically reduces the weight-bearing superior joint space, not the medial |
| Otto pelvis (Fig. 19-4) | Primary protrusio acetabuli; Otto pelvis usually is bilateral and exhibits a female predominance |


GN2 Arthritides
Many disorders cause joint pathology. Arthritides are broadly divided into two groups: those affecting a single joint and those affecting multiple joints (polyarthritis). Polyarthritis can be further divided into inflammatory, degenerative, and metabolic subcategories. Knowledge of the overall prevalence, skeletal target locations, and demography of those affected helps to narrow the long list of etiologies.
Types of arthritis occurring more commonly among men include ankylosing spondylitis, gout, hemophilia, ochronosis, and Reiter syndrome. Common monoarticular arthritides include secondary osteoarthritis (e.g., trauma, avascular necrosis, mechanical stress), gout, and infection. Suppurative arthropathy and rheumatoid arthritis are commonly associated with surrounding osteoporosis. Behçet syndrome, dermatomyositis, Jaccoud arthritis, and Sjögren syndrome characteristically produce transient arthritis, which resolves without residual bone deformity. Joint effusions are pronounced in gout, infection, hemorrhage, and rheumatoid arthritis.
| Disease | Comments |
| Inflammatory (Seropositive) | |
| Jaccoud arthritis (p. 504) | Uncommon, nondestructive arthritis marked by reversible joint derangements, soft-tissue swelling, and pain, classically after an episode of rheumatic fever; Jaccoud arthritis resembles rheumatoid arthritis and affects the joints of the hands and feet |
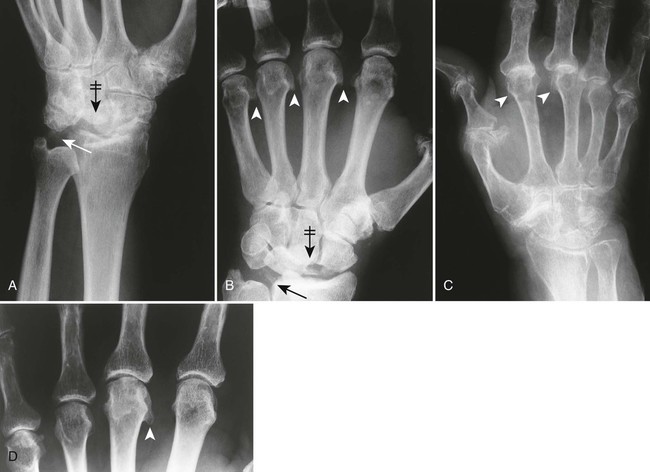
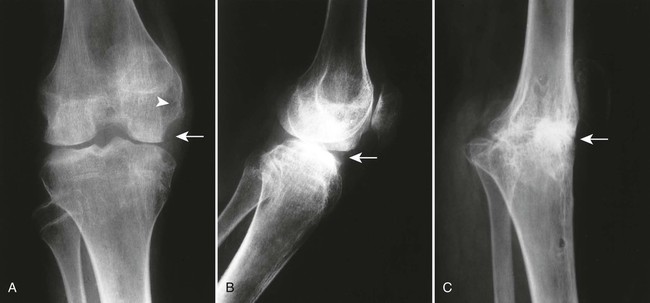
| Rheumatoid arthritis, adult (Figs. 19-5 and 19-6) (p. 480) | Systemic connective tissue disorder targeting synovial tissues; juxtaarticular osteoporosis, soft-tissue nodules, symmetric reduction of joint space, marginal erosions, subchondral cysts, symmetric distribution, and rarely joint ankylosis are characteristic; most commonly, the hands and feet are involved, particularly the intercarpal, metacarpophalangeal, and proximal interphalangeal joints, and counterparts in the foot; rheumatoid arthritis most commonly occurs in middle-aged women |
| Rheumatoid arthritis, juvenile (p. 490) | Chronic arthritis beginning in childhood (before 16 years of age), manifesting as one of several clinical types; monoarticular distribution is more common than in adult rheumatoid arthritis; target areas include cervical spine, hands, feet, and knees; joint fusion, periostitis, and growth abnormalities are characteristic |
| Scleroderma (progressive systemic sclerosis) (p. 498) | Disease of small vessels and organ fibrosis; symptoms include atrophy and systemic dystrophic calcification of the soft tissues of the hands and feet with resorption of distal phalanges; limited soft-tissue swelling, juxtaarticular osteoporosis, marginal erosions, and other similar findings to rheumatoid arthritis occurring in the hands |
| Systemic lupus erythematosus (Fig. 19-7) (p. 496) | Systemic inflammatory connective tissue disease marked by fever, weakness, erythematous skin lesions on the face, and arthritis most visible in the hands as reversible subluxations and dislocations of the digits, predominantly the metacarpophalangeal joints |
| Inflammatory (Seronegative) | |
| Ankylosing spondylitis (p. 505) | Seronegative spondyloarthropathy characterized by arthritis targeted to the sacroiliac joints and spine; bilateral, symmetric, thin intervertebral connections known as syndesmophytes are a prominent feature, representing ossification of the outermost lamellae of the annulus fibrosis; collectively multiple levels produce a “bamboo spine” appearance; in addition, the anterior body margins appear straight or square |
| Psoriatic arthritis (Figs. 19-8 and 19-9) (p. 520) | Arthritis occurs in fewer than 7% of patients with psoriasis; patients experience symptoms in the carpal, interphalangeal, and less commonly the sacroiliac joints; the digits are marked by nail pitting, swelling of the soft tissues, and erosions of the distal tufts, leading to a tapered appearance of the distal phalanges |
| Reiter syndrome (Fig. 19-10) (p. 525) | Describes triad of urethritis, conjunctivitis, and polyarthritis; men, especially those between the ages of 20 and 40 years, contract this condition much more frequently than women; arthritis is targeted to the sacroiliac joints and lower extremities, especially the foot; erosions at the calcaneal insertions of the plantar and Achilles tendons are characteristic |
| Metabolic or Endocrine | |
| Acromegaly (p. 925) | Excess levels of growth hormone result from a pituitary eosinophilic adenoma that is overproducing somatotropin; this condition is marked by progressive enlargement of the hands, feet, head, jaw, and abdominal organs in addition to enlarged vertebrae with posterior scalloping and new bone growth along the anterior body margins; arthritis is targeted to the metacarpophalangeal and hip joints |
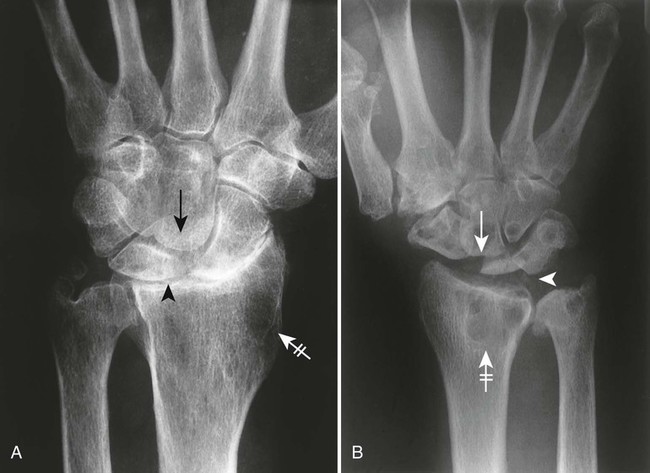
| Chondrocalcinosis (Fig. 19-11) (p. 535) | Radiographically evident cartilage calcification relating to calcium pyrophosphate dihydrate crystal or other crystal deposition disease; chondrocalcinosis is associated with arthritis targeted to the wrist, knees, elbows, hips, and shoulders |
| Gout (p. 530) | Primarily a disorder of purine metabolism with crystal deposits causing synovial pannus, arthropathy, and large well-defined, bony marginal erosions; patients may at times demonstrate sacroiliitis and systemic dystrophic calcifications; typical sites include first metatarsophalangeal joint, insertion of the Achilles tendon, and olecranon bursa |
| Hemochromatosis (Fig. 19-12) (p. 538) | Disorder of iron metabolism resulting from excessive absorption of ingested or injected iron; the disorder is accompanied by cirrhosis of the liver, diabetes, bronze skin pigmentation, generalized osteoporosis, and arthropathy secondary to iron deposits in synovium; the arthritis is targeted to the metacarpophalangeal and interphalangeal joints of the hands; women are protected by menstruation |
| Multicentric reticulohistiocytosis (Fig. 19-13) | Rare disorder marked by cutaneous and joint deposits of histiocytes containing glycolipids; the interphalangeal joints of the hands and feet manifest well-defined marginal erosions; shortening of the fingers often results |
| Ochronosis | Inherited disorder of excessive homogentisic acid production and subsequent accumulation within connective tissues; the spine is affected by multiple levels of intervertebral disc calcification and massive osteophytosis and ankylosis, especially in elderly people; osteoporosis occurs in adjacent vertebrae; advanced degenerative joint disease may develop in the large proximal joints of the extremities (e.g., hip, knee, and shoulder) |
| Degenerative | |
| Erosive osteoarthritis (p. 560) | Seronegative inflammatory variant of osteoarthritis particularly common in 40- to 50-year-old women; proliferative joint changes, central joint erosions, and painful, swollen joints occur; arthritis is targeted to the distal interphalangeal joints of the hands |
| Osteoarthritis (p. 544) | Common, noninflammatory, degenerative joint disease with clinical presentation of pain, stiffness, and crepitus; characteristic radiographic features include bilateral asymmetric distribution, nonuniform reduction of joint space, sclerosis of subarticular bone, marginal osteophytosis, joint malalignment, subchondral cysts, and others; primary osteoarthritis is seen with increasing age and mostly affects weight-bearing joints (e.g., knees, hips, spine) and hands (e.g., distal interphalangeal, first tarsophalangeal, and first carpometacarpal joints); degeneration also occurs secondary to trauma or osteonecrosis |
| Miscellaneous | |
| Hemophilia (p. 779) | Inherited X-linked defect of blood coagulation, marked by a permanent tendency toward hemorrhages; hemarthrosis is associated with red, swollen joints, precocious degenerative arthritis, and an enlargement of the epiphyses; knees, ankles, and elbows are commonly affected; expansile bone lesions (hemophilic pseudotumors) rarely develop; arthritis is targeted to the knees, elbows, and ankles |
| Infection (Figs. 19-14 to 19-17) (p. 789) | Suppurative or tuberculosis infections marked by soft-tissue swelling, juxtaarticular osteoporosis, joint space narrowing, and bone destruction; radiographic findings follow clinical presentation of pain and soft-tissue swelling by 8 to 10 days; infection may affect any joint, most commonly the hip, knee, or spine |
| Neuropathic (Charcot) joints (p. 606) | Destructive arthropathy secondary to altered joint sensory innervation, resulting in either unchecked repetitive injury ensuing from absence of pain or loss of trophic influences of innervations with local hyperemia and bone resorption; atrophic and hypertrophic varieties exist; hypertrophic changes include premature and advanced degeneration, marked by dislocation, destruction, intraarticular loose bodies (debris), and disorganization; this type of arthropathy is common in the knee, hip, ankle, and lumbar spine; etiologies include diabetes, syphilis, syringomyelia, and alcoholism |
| Pigmented villonodular synovitis (p. 875) | Chronic condition marked by diffuse hyperplastic outgrowths of a joint’s synovial membrane; osteolytic appearance results from pressure erosion of adjoining bone; wide age range is possible, although pigmented villonodular synovitis usually occurs before 40 years of age; no juxtaarticular osteoporosis or loss of joint space exists; the most common locations are the knee, hip, ankle, elbow, and shoulder |
| Sarcoidosis (Fig. 19-18) (p. 1240) | Systemic granulomatous disease most pronounced in the lungs; less commonly the disease involves arthritis of the hand with coarsened trabeculae and well-defined osteolytic lesions |
| Others | Transient and episodic arthritis associated with Sjögren syndrome, dermatomyositis, relapsing polychondritis, Behçet syndrome, and so on; patterns of involvement vary |









GN3 Dwarfism
Dwarfism is the condition of being undersized. This condition results from a variety of disorders affecting the growth and development of the tissues. Skeletal dysplasias result in dwarfism because of abnormal tissue development. Skeletal dysplasias are classified according to whether they predominantly affect the proximal or distal long bones of the limb. Rhizomelic (rhiza-, meaning “root,” and –melia, meaning “limb”) dysplasias affect the femur and humerus more so than the tibia or radius. Mesomelic (meso-, meaning “middle”) dysplasia describes shortening of the distal long bones (tibia, ulna, and radius), or middle of the limb relative to the proximal limb (humerus or femur). Acromelic (acro-, meaning “extreme”) dysplasia is a growth disturbance involving the distal portions of the limbs (hands and feet). Micromelic dysplasia involves both the proximal and distal portions of the extremity. Short spine dysplasias cause dwarfism without involving the limbs.
| Disease | Comments |
| More Common | |
| Achondroplasia (Fig. 19-19) (p. 425) | Rhizomelic dysplasia resulting from congenital defect of enchondral bone formation; characteristics include rounded lumbar “bullet-nosed” vertebrae, lumbar kyphosis, posterior scalloping of the vertebrae, increased intervertebral disc height, flattened vertebral bodies, and narrowed spinal canal; the pelvis may appear hypoplastic; milder forms of the disease may occur |
| Less Common | |
| Asphyxiating thoracic dysplasia (Jeune syndrome) (Fig. 19-20) | Mild micromelic dysplasia marked by a small thorax; small, flared iliac bones; and shortening of the humerus, femur (rhizomelia), and distal phalanges (acromelia) |
| Chondrodysplasia punctata | Autosomal dominant (nonrhizomelic) and recessive (rhizomelic) dysplasia; the nonrhizomelic form (Conradi-Hünermann disease) demonstrates tracheal underdevelopment and mild stippled epiphyses; the rarer rhizomelic form is characterized by marked limb shortening, severe punctate calcifications (stippled) epiphyses, metaphyseal splaying, and congenital cataracts |
| Cretinism (p. 934) | Hypothyroid dwarfism from delayed appearance and maturation of skeletal growth centers; stunted mental development occurs; disease appears during the first years of life and results from thymic agenesis or inadequate maternal intake of iodine during pregnancy; wormian bones and poorly developed sinuses are characteristic; sail-like or tongue-like vertebrae and kyphosis at the thoracolumbar junction are common; changes may regress in adulthood |
| Diastrophic dysplasia (p. 434) | Short spine dysplasia characterized by scoliosis, hypoplastic first metacarpal “hitchhiker thumb,” abnormal interphalangeal joints, cleft palate, and clubbed feet |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


