 THE PULMONARY ARTERY
THE PULMONARY ARTERY
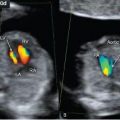
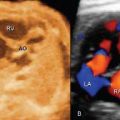
The pulmonary artery (main pulmonary artery, pulmonary trunk) arises from the right ventricle in the anterior aspect of the heart. It crosses over the aorta and points toward the fetal left shoulder as it emerges from the right ventricle. The pulmonary artery, which dips posteriorly into the chest shortly after it crosses over the aorta, divides into the right and left pulmonary arteries and the ductus arteriosus. The ductus arteriosus, which is patent in the fetus, connects with the descending aorta. The division of the pulmonary artery into the right and left pulmonary arteries is an important anatomic characteristic that differentiates it from the ascending aorta. The left pulmonary artery continues posteriorly and inferiorly and courses over the left bronchus into the left lung hilum; the right pulmonary artery originates at a right angle from the pulmonary artery and crosses under the aortic arch, superior to the roof of the left atrium and behind the superior vena cava, before it dips into the right lung hilum. During right ventricular diastole, blood is prevented from flowing back into the ventricle by the pulmonary semilunar valve. The pulmonary semilunar valve is closest to the anterior chest wall, near the left sternal border, and is made of three leaflets: right, left (septal), and anterior. The pulmonary semilunar valve is anatomically separated from the tricuspid valve by a subpulmonic conus. This anatomic separation results in the inability to image both right ventricular inflow and outflow tracts in the same ultrasound plane in long-axis views. In fetal life, the pressure in the pulmonary circulation is near systemic due to the patency of the ductus arteriosus. Prenatally, the thickness of the muscular layer within the wall of the pulmonary tree is similar to that of systemic vessels. Attenuation of this muscular layer is noted in postnatal life due to a decrease in pulmonary arterial pressure that follows closure of the ductus arteriosus.
 THE AORTA
THE AORTA
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


