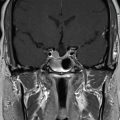
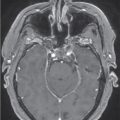
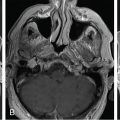
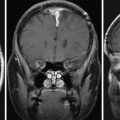
A 30-year-old female sought care after developing persistent galactorrhea following the birth of her first and second children. Preliminary lab work revealed normal prolactin levels but a high level of insulin-like growth factor 1 (IGF-1). Imaging was not sought until a year later when an MRI revealed a pituitary macroadenoma with right cavernous sinus invasion and compression of the optic chiasm ( Figure 3.14.1 ). At this time, her growth hormone (GH) was 2.23 ng/mL, IGF-1 was significantly elevated to 707 ng/mL, and prolactin was slightly elevated to 34.6 ng/mL. The patient reported significantly sharp daily headaches, polydipsia, and polyuria. Formal visual field testing did not reveal any deficits. The decision was made to pursue surgery, during which she underwent endonasal transsphenoidal resection, which was complicated by a cerebrospinal fluid leak that was repaired intraoperatively ( Figure 3.14.2 ). Surgical pathology revealed a pituitary macroadenoma that was immunoreactive for GH. At follow-up, the patient reported improved headaches, decreased frequency of nocturia, and reduced libido. A glucose tolerance test showed a near-normal GH response down to 0.51 ng/mL. However, considering the residual tumor and risk of recurrence, she was referred for Gamma Knife Radiosurgery (GKRS) ( Figure 3.14.3 ).
Radiosurgery Machine
Gamma knife
Radiosurgery Dose (Gy)
25, at 50% isodose line
Number of Fractions
1
Figure 3.14.1.
Initial postcontrast T1-weighted image prior to transsphenoidal resection.
Figure 3.14.2.
Postoperative postcontrast T1-weighted image after transsphenoidal resection.
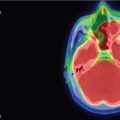
Figure 3.14.3.
Imaging of treatment plan.
Critical Structure
Dose Tolerance
Optic nerve/chiasm
10 Gy maximum point dose
<0.2 cc >8 Gy
Brainstem
15 Gy maximum point dose
<1 cc >10 Gy
Cranial nerves in cavernous sinus
Not fully defined but significantly more resistant than the anterior optic apparatus
Can be more sensitive if SRS follows another type of radiation therapy
Cavernous carotid artery
Very tolerant
Rare cases of asymptomatic carotid stenosis after SRS for pituitary adenomas have been reported
Normal pituitary gland and pituitary stalk
Recommend limiting radiation exposure to the identifiable gland to <11.0 Gy and avoid whole-sella SRS whenever possible
Only gold members can continue reading. Log In or Register to continue



 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
 Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
 Capillary hemangioma – postoperative radiosurgery for residual tumor
Capillary hemangioma – postoperative radiosurgery for residual tumor
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual



