and Hossein Jadvar1
(1)
Department of Radiology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
Cervical Cancer
Case 7.1
History
A 59-year-old female presenting with newly diagnosed cervical carcinoma on biopsy. PET/CT was ordered as a part of the initial treatment strategy evaluation.
Findings
The uterus is anteverted, demonstrating physiologic FDG activity (Fig. 7.1). Intense metabolic activity is seen in the cervical region with associated thickening, SUVmax 16.3, which is compatible with biopsy-proven diagnosis of primary neoplasm. There is a fat plane between the cervix and urinary bladder anteriorly which excludes the direct tumor invasion.

Fig. 7.1
Impression
Cervical thickening demonstrating intense hypermetabolism, which is compatible with biopsy-proven diagnosis of primary neoplasm.
Case 7.2
History
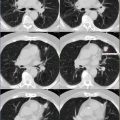
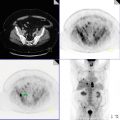
A 51-year-old female with history of cervical cancer.
Findings
1.
There are bilateral supraclavicular, bilateral internal mammary, left axillary, and mediastinal lymph nodes, demonstrating intense FDG activity which is compatible with distant metastatic spread (Fig. 7.2). As a reference, right precarinal lymphadenopathy demonstrates SUVmax 12.9, measuring approximately 2.4 × 3.6 cm, subcarinal lymph node measures approximately 1.7 cm with SUVmax 8.9, left internal mammary lymph node demonstrates SUVmax 7.8, and AP window lymphadenopathy shows SUVmax 10.8.

Fig. 7.2
2.
There is a large hypermetabolic uterine cervical mass demonstrating intense FDG activity, SUVmax 13.8. Exact tumor margins cannot be identified due to lack of IV contrast. There is no fat plane between the tumor and posterior wall of urinary bladder anteriorly, which also abuts the ventral surface of the rectal wall posteriorly, worrisome for local tumor invasion.
3.
There are several hypermetabolic, enlarged retrocrural, retroperitoneal, bilateral common iliac lymph nodes extending inferiorly to involve bilateral external iliac lymph nodes, compatible with metastatic disease. As a reference, left para-aortic lymph node at the level of L1 demonstrates SUVmax 7.5; a right retrocrural lymph node, measuring approximately 1.5 cm at the level of T11 and T12, demonstrates SUVmax 5.5; right common iliac lymphadenopathy also shows SUVmax 5.5; and right internal iliac lymph nodes demonstrate SUVmax 12.1.
4.
Solitary hypermetabolic osseous focus identified at the posterolateral aspect of left eleventh rib, demonstrating SUVmax 5.0.
Impression
1.
Hypermetabolic, large, uterine cervical mass which is worrisome for local tumor invasion.
2.
Metastatic lymphadenopathy involving multiple nodal stations in the neck, chest, abdomen, and pelvis.
3.
Findings compatible with early metastatic disease within the lungs.
Pearls and Pitfalls
1.
FDG PET/CT has no significant role in screening/diagnosis of cervical cancer.
3.
Early response assessments using PET/CT might help to avoid unnecessary and ineffective treatments.
4.
The sensitivity and specificity of PET for early recurrent cervical cancer is 90 % and 76 %, respectively [3].
Discussion
Cervical cancer was once the most common cause of cancer death in women, but the mortality rate has decreased by 50 % due to widespread screening. Worldwide, cervical cancer is the third commonest cancer diagnosed, and it remains the major gynecologic cancer in underdeveloped countries. Squamous cell carcinoma is the most frequent cervical cancer with 85–90 % being invasive. The most common risk factors include lower socioeconomic groups, smoking, early initial sexual activity and/or multiple sexual partners, and history of sexually transmitted disease like gonorrhea, syphilis, and herpes simplex.
MRI is considered the method of choice in the staging of primary tumor since it can evaluate tumor depth and stromal invasion. However, it lacks the ability to accurately diagnose nodal involvement. For this reason, PET is used to assess nodal malignancy as well as regional and distant metastatic disease. Frequency and pattern of cervical cancer lymph node metastasis on FDG PET is influenced by FIGO staging [12, 13]. PET has a 91 % positive value for pelvic and para-aortic lymphadenopathy. In a prospective study on 560 patients, Kidd et al. concluded that the PET findings correlated with the risk of disease progression and survival. In another study looking at the prognostic value of SUVmax, on 73 patients with operable cervical cancer, Chung et al. concluded that FDG tumor uptake correlated with FIGO stage, tumor size, parametrial involvement, and lympho-vascular invasion. These results will likely have important implications for management of cervical cancer patients with lymph node metastasis on FDG PET.
Ovarian Cancer
Case 7.3
History
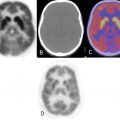
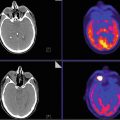
A 61-year-old female with metastatic stage IV ovarian carcinoma, post gamma knife radiosurgery for left frontal and left cerebellar metastasis. PET/CT was done as part of the subsequent treatment strategy evaluation.
Findings
Three hypermetabolic peritoneal implants are seen in the abdomen (Fig. 7.3). These include a hypermetabolic lesion at the hepatorenal surface of segment 6 of the liver measuring 4.2 cm (long axis) with SUVmax 14.8; peritoneum implant in the splenic flexure, measuring 2.0 cm with SUVmax 8.3; and peritoneal implant in the right hemipelvis internal to the right internal iliac vessels showing SUVmax 10.2. Hypermetabolic subcarinal lymph node is seen with increase in size and activity, SUVmax 8.2. Physiologic brown fat activity is seen in the superior mediastinal and bilateral paravertebral regions.

Fig. 7.3
Impression
Three peritoneal implants with increased size and metabolic activity.
Case 7.4
History
A 53-year-old female with stage IV ovarian carcinoma, status post hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and bilateral lymph node dissection with appendectomy, currently on chemotherapy (Taxol). PET/CT was done as part of subsequent treatment strategy evaluation.
Findings
Overall, previously seen majority of the hypermetabolic abdominal lymph nodes have resolved (Fig. 7.4). Exceptions include a porta hepatis lymph node which has decreased in FDG activity and currently demonstrates SUVmax 6.5, previously 9.5; a mesenteric lymph node near the terminal ileum has increased in FDG activity and currently demonstrates SUVmax 12.1 previously 9.3. Additionally, there is a new right retrocrural lymph node which currently demonstrates SUVmax 8.6.

Fig 7.4
Impression
1.
Resolution of majority of hypermetabolic abdominal and chest lymph nodes with the exception of the porta hepatis lymph node and mesenteric lymph node adjacent to the terminal ileum.
2.
New hypermetabolic right retrocrural lymph node.
3.
Overall findings consistent with a substantial partial response to interval chemotherapy.
Case 7.5
History
A 65-year-old female with ovarian cancer, currently on chemotherapy.
Findings
Multiple hypermetabolic omental/peritoneal metastases are seen, like the peritoneal implant lateral to psoas in the left iliac fossa with SUVmax 9.3 (Fig. 7.5). The lymph nodes are involved which are intensely hypermetabolic, for example, retroaortic node at L4 with SUVmax 12.3, left common iliac with SUVmax 8.8, left external iliac with SUVmax 7.1, and left hypogastric with SUVmax 5.7.

Fig. 7.5
Impression
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


