Head and Neck Squamous Cell Cancer with Nodal Metastases
Benjamin Y. Huang
CLINICAL HISTORY
57-year-old male presenting with an enlarging right neck mass and progressive dysphagia.
 FIGURE 65A |
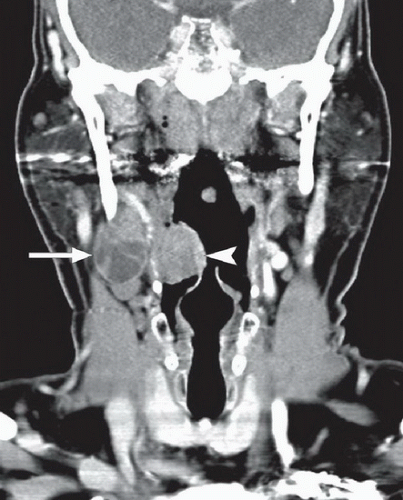 FIGURE 65B |
FINDINGS
Figures 65A and 65B: Axial (Fig. 65A) and coronal (Fig. 65B) contrast-enhanced CT images of the neck demonstrate an ovoid mixed solid and cystic density mass in the right neck (arrow) situated just inferior to the mandibular angle and anteromedial to the sternocleidomastoid muscle. In addition, there is increased and asymmetric soft tissue situated along the right tongue base and lateral pharyngeal wall (arrowhead).
DIFFERENTIAL DIAGNOSIS
When faced with a new neck mass in a patient over the age of 40 years, malignancy should be considered the primary diagnosis until proven otherwise, and in this case, metastatic lymphadenopathy from an oropharyngeal cancer should be the main concern. Other neoplastic causes of cervical lymphadenopathy include metastases from cancers of the skin, parotid gland, and thyroid, as well as lymphoma. In children and adults under the age of 40, the majority of posterior and lateral neck masses represent inflammatory lymphadenopathy (although the likelihood of neoplasm goes up with increasing age). Infectious causes of lymph node enlargement include suppurative bacterial adenitis, mycobacterial (tuberculous and nontuberculous) lymphadenitis, cat scratch disease, and actinomycosis. These entities can all present with cystic or necrotic lymphadenopathy. A second branchial cleft cyst can also present as a cystic mass in this location; however, these usually present in childhood and should not demonstrate significant soft tissue elements or enhancement, although they may show peripheral enhancement if infected.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


