Anirudh Kohli Imaging plays an important role in the early detection, characterization and management of infectious liver disease. Prompt diagnosis and management are crucial, especially for pyogenic and fungal infections because they can be fatal if not treated early. Ultrasonography (US), computed tomography (CT) and magnetic resonance (MR) imaging allow accurate detection of most hepatic infections, sometimes providing clues to identify the underlying pathogen. Liver abscess is the most common type of visceral abscess. The pathogenesis of liver abscesses is multifactorial: Most pyogenic liver abscesses are polymicrobial. Traditionally, Escherichia coli has been reported as the most common isolated microbe; however, recent data show that Klebsiella pneumoniae is also a common pathogen in pyogenic liver abscesses. Clinical manifestations include a broad spectrum of symptoms, but the most common are fever and abdominal pain, usually in the right upper quadrant. Management of pyogenic liver abscesses includes imaging-guided drainage and antibiotic therapy. It is recommended that antibiotic therapy be continued for at least 4–6 weeks, but the optimal duration is still unclear. Although drainage of single abscesses with a diameter of 5 cm or less can be achieved, it may not improve outcomes compared with antibiotic treatment alone. In isolated abscesses with a diameter greater than 5 cm, aspiration or catheter drainage should be considered. Prompt diagnosis and imaging-guided drainage have been reported to reduce mortality. Sonography is usually the first line of investigation. Its sensitivity is 85%. Small abscess (<2 cm) appear as hypoechoic nodules or ill-defined areas of distorted hepatic echogenicity. Large abscesses range from hypoechoic to hyperechoic masses, depending on the presence of internal echoes or due to debris. Occasionally they appear very echogenic resembling solid lesions especially if they are of K. pneumoniae aetiology. In the initial phase of development of an abscess before liquefaction has occurred abscess may be solid and mimic a neoplasm. Multifocal liver abscess may mimic metastases. Clinical history of fever, abdominal pain, leukocytosis are critical in making the diagnosis. As liquefaction occurs the cystic nature of abscess becomes more apparent. Doppler may show hyperaemia around the abscess. CT has a much higher sensitivity of 97% in detecting a hepatic abscess. On contrast-enhanced CT abscess appear as a well-defined, low-attenuation, round lesion with an enhancing peripheral rim. They may be single unifocal, single multiloculated lesions or multifocal lesions. The ‘double target sign’ is a characteristic imaging feature of hepatic abscess seen on contrast-enhanced CT images when a central low-attenuation fluid-filled area is surrounded by a high-attenuation inner ring and a low-attenuation outer ring. The inner high attenuation layer shows early contrast enhancement that persists in delayed phases, as opposed to the outer layer, which is low attenuating in the early arterial phase and enhances only in delayed phases. The inner layer represents the pyogenic membrane, and the outer layer is due to oedema of the hepatic parenchyma. The ‘cluster sign’ is also an imaging feature of pyogenic abscesses and occurs when multiple small low-attenuation lesions aggregate in a localized area and coalesce into a single larger abscess cavity. There is usually also a wedge-shaped or circumferential segmental region of hepatic hyperenhancement in the late arterial phase, which becomes isodense on the portal and delayed phases. This occurs due to compression off small portal venules surrounding the hepatic abscesses, which results in reduction of portal flow and a compensatory increase in arterial inflow. Also termed as transient hepatic attenuation or signal intensity difference, this is also seen in tumours. MR: abscesses typically show central low T1-weighted and high T2-weighted signal intensity, though internal signal intensity may vary depending on the protein content. The double target sign is also seen on T2-weighted images as an iso- to hypointense inner layer and a hyperintense outer layer. There is early enhancement of the inner layer that persists in the delayed phase, and delayed enhancement of the periphery. Diffusion-weighted imaging is very important in liver abscess. The internal contents are bright on diffusion images and demonstrate marked hypointensity on ADC. This is a very important feature to differentiate abscess from necrotic tumours. Both lesions, an abscess as well as a necrotic tumour will appear similar, hyperintense on T2, hypointense on T1 with peripheral enhancement as well as transient hepatic intensity difference around the lesion. ADC will differentiate between a necrotic tumour and an abscess. Abscess contents will be hypointense, dark on ADC whereas necrotic component of tumour would be hyperintense on ADC. Twenty per cent of abscesses may contain specs of air or a fair amount of gas resulting in an air-fluid level. Air is best appreciated on CT. On sonography air is seen as small echogenic specs with posterior acoustic shadowing/reverberations. On MRI gas appears as signal voids within an abscess best seen on T1WI, gradient-echo images or in-phase images. Absorbable hemostátic material placed after surgical interventions such as hepatic resection, transplantation to contain excessive bleeding may look like a complex fluid collection with focal pockets of air within resembling an abscess. These may persist for up to one month. Differentiation from an abscess occurs based on the clinical data of the type of surgical procedure performed. Cholangitic micro abscess may appear similar to cysts as they are small well defined and T2 hyperintense. They however reveal wall enhancement, perilesional oedema, diffusion restriction and associated marked segmental enhancement. Cholangitic abscess are also symptomatic with right upper quadrant pain, fever as compared to biliary cysts hamartomas which are asymptomatic. The segmental enhancement often brings them to attention as the abscesses are very small. This parasitic disease is caused by the larva of tapeworms. Dogs or carnivorous animals are the definitive hosts, humans are the intermediate host. Humans are infected by ingestion of food or water contaminated by dog faeces containing tapeworm eggs. The ingested embryos invade the intestinal mucosa and enter the portal circulation. Most of the embryos are filtered in the hepatic capillaries, most of these die, a few form Hydatid cysts. Some of the embryos may pass through the hepatic capillaries and become lodged in the lungs and other organs. This is usually eosinophilia, serological testing is only positive in 25% of patients, therefore, imaging is very important in establishing a diagnosis of hydatidosis.
9.13: Hepatic infections
Introduction
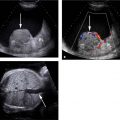
Pyogenic abscess
Imaging
Hydatid disease
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


