ISOMERISM, RIGHT ATRIAL
ISOMERISM, AND SITUS INVERSUS
22
 FETAL HETEROTAXY WITH LEFT ATRIAL ISOMERISM AND RIGHT ATRIAL ISOMERISM
FETAL HETEROTAXY WITH LEFT ATRIAL ISOMERISM AND RIGHT ATRIAL ISOMERISM
Definition, Terminology, and Incidence
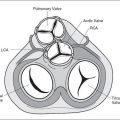
The embryologic development of abdominal and thoracic structures follows a spatially controlled and coordinated manner leading to well-defined right-sided and left-sided anatomic positions within the body. Right-sided structures include a major part of the liver, the inferior and superior vena cava, the right atrium with its appendage, and a trilobed right lung with an eparterial bronchus (see Table 4-1). Left-sided structures include the stomach, the spleen, the left atrium with its appendage, the pulmonary veins, and a bilobed left lung with a hyparterial bronchus (see Table 4-1). Normal development and positioning of abdominal and thoracic organs is referred to as situs solitus (solitus means common) for the visceral arrangement, and levocardia (heart on the left side) for the thoracic arrangement of organs (1–3). Situs inversus refers to a mirror-image arrangement of the visceral and thoracic structures to that of situs solitus. Any arrangement of visceral and/or thoracic organs other than situs solitus or situs inversus is referred to as situs ambiguous (unknown or complex situs). Situs ambiguous, unlike situs solitus or inversus, is often associated with various anomalies including anomalies of the spleen, either as asplenia or polysplenia. The term cardiosplenic syndrome was first used to describe situs ambiguous associated with anomalies of the spleen. Since the spleen is not always abnormal in situs ambiguous and cannot be reliably used for classification, the term heterotaxy syndrome has been suggested (1,2). Heterotaxy syndrome (in Greek, heteros means different and taxis means arrangement) is a general term that is used to describe the complete spectrum of abnormal organ arrangement including conditions such as asplenia and polysplenia. Since many pathologists observed that the subgroups of asplenia and polysplenia are better classified by describing the atrial morphology, the term right and left atrial isomerism (in Greek, iso means same and meros means turn) has been suggested and used (4) (Fig. 22-1A–C). Heterotaxy of the abdominal organs involves an irregular arrangement of the nonpaired solitary organs. Heterotaxy of the thoracic organs is characterized by a rather symmetric arrangement of the otherwise asymmetric structures including the atria and lungs (3), thus allowing a classification into two main groups: bilateral right-sidedness, also called right atrial isomerism (asplenia, Ivemark syndrome), and bilateral left sidedness, also called left atrial isomerism (polysplenia).
Heterotaxy syndrome is found in between 2.2% and 4.2% of infants with congenital heart disease (5,6). In fetal series, left isomerism is more common than right isomerism. In postnatal series, right isomerism is more common owing to an increased incidence of in utero demise of fetuses with left isomerism due to complete heart block and hydrops (3). Fetal heterotaxy has an increased risk of recurrence in subsequent pregnancies, and that risk has been reported in up to 10% in some series (7). A genetic etiology for heterotaxy recurrence that may include autosomal dominant, autosomal recessive, X-linked, and single gene disorder has been suggested (8–10). Recurrence of heterotaxy in families is not limited to the specific anomaly but may involve the full spectrum including right or left isomerism and situs inversus.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


