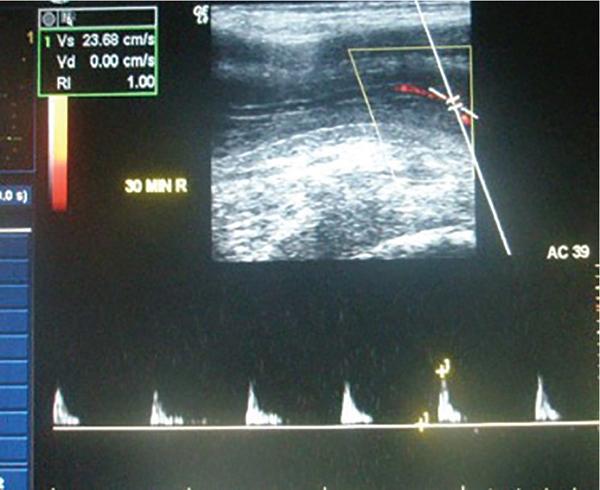
Rijo Mathew Choorakuttil The penis is a superficial, protruding organ that is highly vascularized and composed of several soft tissue structures. Penile pathologies and abnormalities are not uncommon, although they are not usually as well discussed as other organ pathologies. Ultrasound studies are useful in the assessment of penile pathologies and dysfunctions. In this chapter, you will learn about Penile erection is primarily a neurovascular phenomenon, initiated by erection triggers such as imagination, visual, auditory, olfactory, genital and nongenital tactile stimulation. These triggers result in neurologic signals transmitted through the parasympathetic nerves and release of nerve-derived nitric oxide (nNOs) and vasodilatation. Due to the vasodilatation, endothelium-derived nitric oxide (eNOs) is produced, which continues to produce vasodilatation if the erection triggers are continuously operating and facilitated only in the presence of a hormonal and psychological environment. Sexual stimulation initiates the release of neurotransmitters from the cavernous nerve terminals and relaxing factors from the endothelial cells result in arteriolar smooth muscle relaxation. Increased blood flow and relaxation of the cavernous smooth muscle result in rapid filling and enlargement of sinusoids against the TA. The compression of the subtunical venular plexuses lead to a significant occlusion of venous outflow. Blood is trapped within the cavernosa and raises the intracavernosal pressure (ICP). This leads to full erection. The base of the corpus cavernosum, which is blood filled, is compressed by the ischiocavernosus muscle during sexual activity. The penis enters the rigid erection phase with temporary cessation of the inflow and outflow. Emissary veins get contracted between the circular and oblique fibres of tunica to maintain the blood filled in sinusoids in erection. Detumescence begins as the trabecular smooth muscle contracts and venous channels open, expel the trapped blood and restore flaccidity. The penis is an organ given to intermittent tumescence that is often related to sexual stimulation. Priapism is a persistent tumescence unrelated to sexual stimulation that usually lasts more than 4 h. Priapism can be categorized as arterial and venous types. Arterial priapism is less common that venous or ischemic priapism. Ischemic priapism, caused by decreased or absent venous drainage is a medical emergency that needs immediate attention. Arterial or high-flow priapism is often seen in fistula formation or cavernosal metastasis of a solid tumour and is caused by arterial influx that is increased and often uncontrolled. Arterial-lacunar fistula seen in arterial priapism may directly extend to the cavernosal tissue and bypass the helicine arteries. Colour Doppler ultrasound (CDUS) studies reveal a characteristic colour blush and turbulent high-velocity flow. Low-flow or ischaemic priapism occurs as a failure of tumescence characterized by the absence of cavernosal blood flow. Low-flow priapism commonly reveal a lack of CA blood flow or with a very high-resistance flow pattern in the CA in CDUS. Progressive curvature and shortening of the penile shaft are the characteristic of Peyronie’s disease. It may be associated with a palpable nodule and may lead to pain during erection and dyspareunia. Penile ultrasound imaging studies may show multiple calcified nodules along the tunical envelope of the cavernosum and signs of veno-occlusive erectile dysfunction (ED) (Fig. 11.13.1). Improvements in real time spatial resolutions and contrast have helped in the preoperative assessment of Peyronie’s disease and the quantification of penile fibrosis. Sonoelastography and contrast-enhanced penile ultrasound studies can also help to provide more information on penile pathology. Sonoelastography techniques are useful to differentiate and detect noncalcified fibrous plaques. ED may be psychogenic, organic or of mixed aetiology. Reliable estimates on the exact prevalence of ED is scarce, although some studies have reported a prevalence of 12% in men aged above 18 years and 25%–30% in men aged between 60 and 70 years and 52% in the Massachusetts Male Aging Study. Nearly 70% of men may suffer from ED at some time during their life and 30% of men may experience one episode of ED in a given month. Estimates suggest that an estimated 152 million men worldwide were present with ED in 1995 and this may increase to nearly 322 million men with ED by 2025. ED can cause stress, affect self-image and cause lack of confidence as well as relationship problems. ED can also suggest an underlying health condition that needs treatment. ED is one of the earliest manifestations of endothelial dysfunction and peripheral vascular and cardiovascular disease in men. Vascular insufficiency and ED secondary to excessive venous leakage is the most common cause of organic ED. Persons with ED of vascular causes have more markedly impaired endothelial and smooth muscle functions compared with patients having similar risk factors but no ED. The prevalence of vascular comorbidities increased with ED severity suggesting that ED may be a prognostic marker for overall health. ED is an important legal question especially in cases or marital consummation, separation and divorce and rape and sexual assault. Doppler ultrasound studies may be useful in the determination of ED in such cases. The treatment of structural penile diseases depends on the underlying causes. Medical therapy may help in patients with moderate disease while surgical correction may be needed for persons with severe penile deformity. It is possible to minimize the diagnosis of indeterminate cause with proper ultrasound techniques and interpretations. The determination of psychogenic ED is important and appropriate counselling and psychotherapeutic processes may help to alleviate symptoms in psychogenic ED. Penile trauma is relatively rare, but not uncommon and has a reported incidence of 1 in 175,000 hospital admissions. Rupture of the TA and the corpus cavernosa, often seen in the setting of an erect penis during vigorous sex, direct trauma, masturbation, falls, forceful manipulation and rolling over in bed during an erection, can lead to penile fractures (PF). PF may need emergency surgical repair. On the other hand, blunt penile injury without disruption of the TA or urethral injury may be treated conservatively. The TA, which has a normal thickness of 2 mm in a flaccid penile state elongates during erection with a reduction of thickness to 0.25 mm. A transverse rupture of the corpus cavernosum can lead to a curved or bent penis. Penile fracture generally occurs in the proximal or middle shaft and results in a transversal tear. Radiologic evaluation for PF includes retrograde urethrography, cavernosography, magnetic resonance imaging (MRI), US and CD ultrasonography. Retrograde urethrography and cavernosography are invasive and with high rates of false-negative findings. MRI is an excellent imaging modality with multiplanar capability and excellent tissue contrast but is expensive and not widely available everywhere. US is ideal to evaluate patients with penile trauma and can be routinely used in an emergency. It is a noninvasive method and should be performed with a high-frequency (7–12 MHz) linear transducer, anatomic orientation and ample gel to provide high-quality images. Ultrasound studies that use high-resolution greyscale imaging, high-frequency broadband traducers, in isolation or with colour and pulsed-wave Doppler are the initial tests for the evaluation of penile trauma. Colour duplex Doppler ultrasound (CDDU) is performed using a high-resolution probe – range of 10 to 16 MHz positioning the probe at the crus (at the level of penoscrotal junction) and at mid penis (1/2 distance between the penoscrotal junction and the coronal sulcus). Vasoactive drugs (intracavernosal injection of papaverine 60 mg (n = 700) or prostaglandin E-1 20 mcg, n = 1576), audiovisual sexual stimulation (AVSS) and/or tactile sexual stimulation (TSS), in a quiet room with aesthetic and erotic environment and without any external disturbances are part of the assessments as appropriate. The assessments are done in the presence of a team that included andrologist, radiologist and sex therapist. Sampling factors, gate placement and angle corrections are optimized for consistent, reproducible results. The penis is scanned from its ventral surface using longitudinal and transverse views. Evaluation is done with the penis in a flaccid state and after the intravenous injection of the vasoactive drugs. CDUS with spectrum analysis is performed with tuning for a slow-flow setting. Penile bodies present with intermediate echogenicity and homogeneous echotexture in the flaccid state. After a cavernosal injection, sinusoidal distension begins in the central portion of the cavernosa and is less echogenic than the outer portion. The filling phase reveals several fine echogenic grids of the sinusoidal interfaces in the corpus cavernosum. The penile septum is a back attenuated echogenic structure that may obstruct the evaluation of the dorsal penis and the TA. The sampling location and angle can influence the measurement of the peak systolic velocity (PSV) of the CA (Fig. 11.13.2). Colour Doppler signals are used to guide spectral sampling of the CA at the origin on the base of the penis, at the site where CA angles posteriorly toward the crus. This helps to standardize velocity measurements. It is preferable to apply the angle correction cursor or the steering box (Fig. 11.13.3).
11.13: High-resolution ultrasound and colour doppler in penile pathologies and erectile dysfunction
Learning objectives
Anatomy of the penis in ultrasound imaging
Soft tissue structures
The penile blood supply
Penile erection
Common penile pathologies
Priapism
Peyronie’s disease

Erectile dysfunction
Penile trauma and fractures
Ultrasound assessments of the penis
For erectile dysfunction
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


