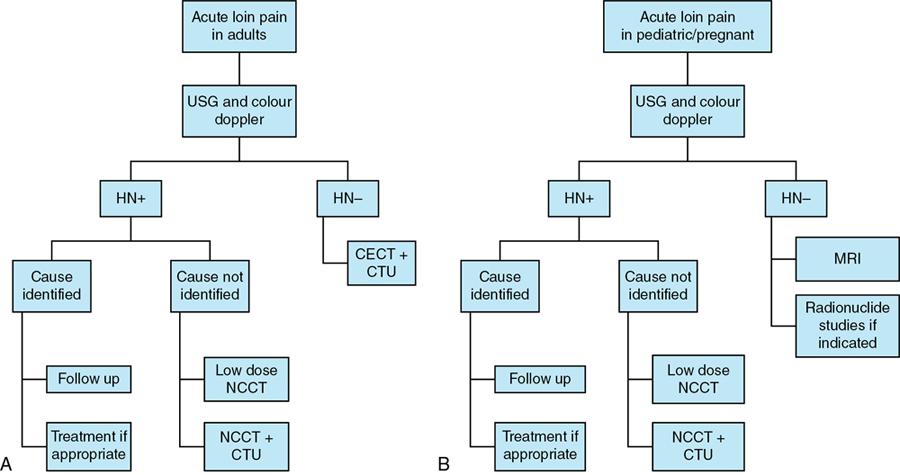
Hydronephrosis refers to the dilatation of renal pelvis and calyces. It can result from both obstructive and nonobstructive pathologies in the urinary tract. Obstructive hydronephrosis is more commonly encountered and urinary tract calculi represent the most common cause of obstruction in adults. Hydronephrosis is commonly associated with some amount of ureteric dilatation (hydroureter); however, isolated hydronephrosis may be seen when the obstruction is at the level of pelviureteric junction. Obstructive uropathy refers to the structural and functional abnormalities in the urinary system resulting from obstruction. It has been observed that obstructive nephropathy can rarely present without hydronephrosis. Patients with obstruction are prone to develop urinary infections and renal failure. Hence early diagnosis is essential to prevent irreparable damage to the urinary tract. Obstructive hydronephrosis: The causes of obstructive dilatation can be categorized based on the level of obstruction and are enumerated in Box 10.12.3.1.1. CAUSES OF OBSTRUCTIVE HYDRONEPHROSIS Nonobstructive hydronephrosis (enumerated in Box 10.12.3.1.2): CAUSES OF NONOBSTRUCTIVE HYDRONEPHROSIS The changes in the renal structure and function depend on the level, extent and duration of the obstruction within the urinary tract. Urinary obstruction may present with nonspecific symptoms. Loin pain is usually the most common presentation in acute urinary obstruction. Renal and ureteric pathologies result in referred pain in the loin region. It may be associated with renal angle tenderness, nausea, vomiting and microscopic haematuria in calculus disease. Sometimes renal failure may be the initial presentation in patients with underlying disease or sepsis. Patients with chronic obstruction may remain asymptomatic. Imaging in patients with acute loin pain is aimed at not just identifying the cause of obstruction, but also the level and extent of obstruction and potential complications. The role of intravenous urography (IVU) as the primary imaging modality in suspected urinary obstruction has been superseded by the development of low dose noncontrast CT (NCCT) examination. The main advantage of IVU was the ability to determine both anatomic and functional alterations in the kidney secondary to obstruction. However, IVU requires serial delayed images to assess renal function which is cumbersome in an acute setting. Contrast-induced nephropathy is another potential concern with IVU which can be overcome using renal ultrasound and NCCT. CT urography has emerged as the imaging technique of choice in the evaluation of acute urinary obstruction due to both structural and functional assessment. The algorithm for the evaluation of patients with acute loin pain is depicted in the flow chart (Fig. 10.12.3.1.1). A supine radiograph of the kidney, ureter and bladder (KUB) region can identify radiopaque calculi. Most of the calculi are calcium-containing and radiopaque. Radiolucent calculi containing uric acid, xanthine and other metabolic constituents are missed. Acute obstruction can be diagnosed on IVU from the following signs (Fig. 10.12.3.1.2):
1. Hydronephrosis and obstructive uropathy
Introduction
Aetiology
OBSTRUCTION AT THE LEVEL OF URETER
Congenital
Acquired
Stricture
Intraluminal
Ureterocele
Calculus
Pelviureteric junction obstruction
Blood clot
Sloughed renal papilla
Fungal ball
Foreign material
Intramural
Neoplastic
Epithelial and nonepithelial tumours
Metastasis
Infective/Inflammatory
TB ureteritis
Schistosomiasis
Ureteritis cystica
Malacoplakia
Leucoplakia
Radiation ureteritis
Extrinsic
Hydronephrosis of pregnancy
Retroperitoneal fibrosis and tumours
Pelvic lipomatosis
Pelvic tumours
Gynaecological causes
Gastrointestinal conditions
OBSTRUCTION AT THE LEVEL OF URINARY BLADDER AND URETHRA
Congenital
Acquired
Posterior urethral valve
Benign
Hypospadias
Benign prostatic hypertrophy
Neurogenic bladder
Neoplastic
Carcinoma bladder
Carcinoma prostate
Pathophysiology
Clinical features
Diagnostic imaging
Plain radiograph
Intravenous urography
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


