Hypopharynx: Benign Noninflammatory Masses and Tumors
KEY POINTS
- Computed tomography and magnetic resonance imaging are quite valuable diagnostic tools for the evaluation and planning of the next steps in the diagnosis management of submucosal hypopharyngeal masses that are eventually shown to be benign.
- Such imaging can help to avoid possible complications, such as excessive bleeding from endoscopic biopsy.
After physical examination, it is often difficult to decide whether an area of swelling is neoplastic, inflammatory, traumatic, or degenerative. Even after biopsy, the etiology may remain obscure.
Most benign tumors or focal areas of swelling in the hypopharynx will have a nonspecific imaging appearance. On occasion, imaging findings will be specific enough to allow an etiologic or, rarely, a very likely specific tissue diagnosis. The most fitting and usual use of computed tomography (CT) and magnetic resonance imaging (MRI) is to show the extent of the lesion and identify the likely etiology of a submucosal mass.
ANATOMIC CONSIDERATIONS
Applied Anatomy
A thorough knowledge of hypopharyngeal anatomy and anatomic variations in each of the following areas is required for the evaluation of benign, noninflammatory masses of the hypopharynx. This anatomy is presented in detail with the introductory material on the hypopharynx, larynx, cervical esophagus, and infrahyoid neck in general.
Evaluation of the hypopharynx and related structures frequently involved with contiguous disease in these conditions should include the following:
- Hypopharynx, including its three components: the posterior pharyngeal wall, pyriform sinus, and postcricoid portions (Chapter 215)
- Larynx, including the laryngeal skeleton, deep tissues spaces within the larynx, mucosal landmarks, and functional structures within the larynx (Chapter 201)
- Tongue base region and low oropharyngeal wall (Chapter 190)
- Cervical esophagus and its junction with the postcricoid portion of the hypopharynx (Chapter 221)
- Trachea (Chapter 209)
Evaluation of Extrapharyngeal Spread
- Visceral compartment of the neck and related fasciae (Chapter 149)
IMAGING APPROACH
Techniques and Relevant Aspects
The hypopharynx is studied in essentially the same manner for benign masses of known or uncertain etiology as it is for the evaluation of known or suspected laryngeal cancer. The principles of using these studies are reviewed in Chapters 201 and 206. Specific problem-driven protocols for CT and MRI of the larynx and hypopharynx are presented in Appendixes A and B, respectively.
There is little or no use for ultrasound in studying these masses.
There is a limited role for catheter angiography in lesions where the physical examination and imaging with CT angiography and/or MRI suggests that they are vascular in origin or very hypervascular.
Radionuclide studies are generally not useful in benign masses of the hypopharynx, except perhaps to confirm the presence of a neuroendocrine lesion under very unusual circumstances.
Pros and Cons
Evaluation of Submucosal or Other Masses of Uncertain Etiology
Benign masses limited to the hypopharynx often mimic the initial presentation of hypopharyngeal cancer. Frequently, both the larynx and hypopharynx will be involved, especially in lesions that arise within the aryepiglottic fold (Figs. 218.1–218.4). Any mass, regardless of etiology, that is suspicious for deep infiltration or cancer should be studied primarily with CT if imaging is desired as part of the evaluation. MRI can be used initially if preferred but is much more likely to be significantly degraded and sometimes nondiagnostic due to motion artifacts. Supplemental magnetic resonance (MR) study, in the situations where it might add meaningful incremental data, is best directed by CT findings to a localized area of interest where its strengths related to better soft tissue contrast resolution may be exploited.
Integrity of the Airway
In any imaging study of the hypopharynx, the diseased condition must be evaluated for its effect on the airway. The anatomic status of the airway, as well as the risk of any acute adverse complication, such as the potential for rapidly progressive airway obstruction either by the mass or a potential airway complication that might arise as a result of biopsy, should be reported. For instance, biopsy of an unanticipated paraganglioma or vascular malformation could lead to an unfortunate amount of hemorrhage and aspiration of blood (Figs. 218.5–218.7).
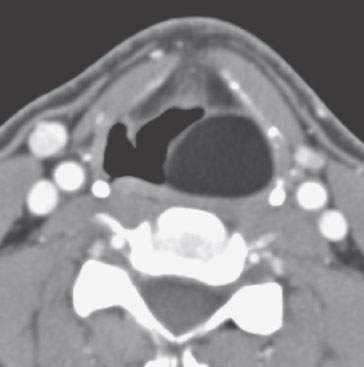
FIGURE 218.1. Axial computed tomography images through the larynx show a well-demarcated lipoma in the left aryepiglottic fold extending into the paraglottic space and pyriform sinus. (Courtesy Frank Pameijer, Utrecht, The Netherlands.)
Evaluation of Pharyngeal Dysfunction Possibly Due to Submucosal Masses
Some patients have processes predominantly occurring beneath intact hypopharyngeal mucosa that cause dysphagia, odynophagia, and/or aspiration. Imaging is particularly valuable to the head and neck surgeon to better delineate the submucosal extent of a lesion that may spread underneath intact and normal-appearing mucosa. In such circumstances, endoscopic examination of the upper aerodigestive tract can often underestimate the size of the lesion, further complicating surgical planning (Fig. 218.8). Sometimes, a clinically submucosal mass does not originate from the hypopharynx itself but from some of the neighboring structures, causing secondary compression of the hypopharynx (Fig. 218.9).
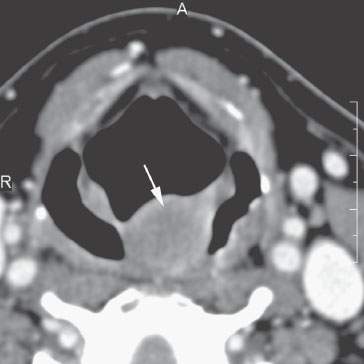
FIGURE 218.2. Contrast-enhanced computed tomography of a patient with a polypoid mass along the low oropharyngeal and upper hypopharyngeal wall that subsequently proved to be a rhabdomyoma or low-grade rhabdomyosarcoma (arrow).

FIGURE 218.3. Axial computed tomography image showing exophytic tumor with a low-attenuating periphery and enhancing inner part originating from the aryepiglottic fold. This turned out to be a schwannoma. (Courtesy Marie-Madeleine Plantet, Saint-Cloud, France.)
Vocal Cord Dysfunction and Weakness
Benign hypopharyngeal masses, especially those that are at the apex of the pyriform sinus, can affect true vocal cord (TVC) function. Imaging can be useful in showing a likely benign mass as the cause for such TVC dysfunction (Fig. 218.8).
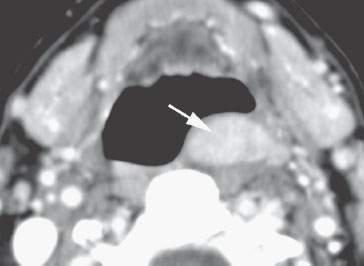
FIGURE 218.4. Patient presenting with a neck mass. Imaging revealed multiple lesions, with biopsy showing them to be multiple granular cell tumors. One of several images shown in Figure 30.15 of a submucosal mass due to one of the granular cell tumors this one at the junction of lower posterior oropharyngeal and upper hypopharyngeal walls.
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


