HYPOPHARYNX: INTRODUCTION, NORMAL ANATOMY, AND FUNCTION
IMAGING APPROACH
Techniques and Relevant Aspects
The hypopharynx is studied in essentially the same manner as the larynx; therefore, the principles related to imaging of the hypopharynx with computed tomography (CT) and magnetic resonance (MR) should be reviewed in Chapter 201. Specific problem-driven protocols for CT and MR are presented in Appendixes A and B.
There is little or no use for ultrasound in studying the hypopharynx except in practices that use this imaging to assess lymph node disease in patients with hypopharyngeal cancer.
The approach with radionuclide studies depends on the aim of the examination. Most of the current usage is limited to cancer evaluation with fluorine-18 2-fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET). This is discussed in more detail in conjunction with the larynx in Chapters 201 and 206.
Pros and Cons
Indications for Study
Evaluating the Extent of Known Hypopharyngeal Cancer and Related Regional Lymph Node Metastases and Posttreatment Surveillance
This is discussed more fully in conjunction with laryngeal cancer in Chapter 206.
Evaluation of Submucosal or Peripharyngeal Masses of Uncertain Etiology
Both CT and MR can be used to demonstrate the presence, nature, and extent of a submucosal mass lesion. In most cases, a CT study is adequate for all of these tasks. A variety of sometimes unusual lesions, either benign or malignant, can be encountered in this clinical context. As the initial biopsy results may be inconclusive or negative, MR may be used in an attempt to further characterize the lesion. In young patients, MR might be preferred because of the absence of ionizing radiation.
Throat Pain, Referred Otalgia, Dysphonia, and Vocal Cord Dysfunction
CT is the preferred modality for these studies since it not only provides a good evaluation of the hypopharynx and larynx but also can easily be extended to include the upper thoracic cavity or intracranial structures in cases of potential vagus nerve dysfunction. Adjunctive magnetic resonance imaging (MRI) may be used selectively to evaluate the cisternal course of the vagus nerve and its brain stem nuclei.
Pharyngeal Trauma
CT is the preferred modality for the study of pharyngeal trauma, as it can be performed more simply than MRI in the acute or immediate subacute clinical setting and provides superior cartilage detail and multiplanar images. It simultaneously allows a thorough evaluation of the other neck structures, including soft tissue injury that might be associated with pharyngeal tears, vascular injury, and cervical spine injuries, among others. It is also better for identifying gas and retained foreign bodies; this is especially useful in the evaluation of a potentially swallowed foreign body.
Functional Studies
Water-soluble contrast and barium studies remain the preferred studies for gross screening for perforations or false passages, functional disorders, and mucosal lesions.
Controversies
There is some debate with regard to whether CT or MR should be the primary imaging tool for evaluating patients with hypopharyngeal cancer. This discussion often emphasizes which study is best at showing cartilage involvement and is discussed in detail in conjunction with laryngeal cancer evaluation in Chapter 206.
NORMAL ANATOMY
General Description
The hypopharynx is an inferior continuation of the pharynx. The pharynx is essentially a muscular tube suspended from the skull base, and it is useful to recall the general anatomy of the upper pharynx when thinking about its lowermost segment, the hypopharynx. The three components of the hypopharynx are the posterior pharyngeal wall, the pyriform sinuses, and the postcricoid region (Fig. 215.1).
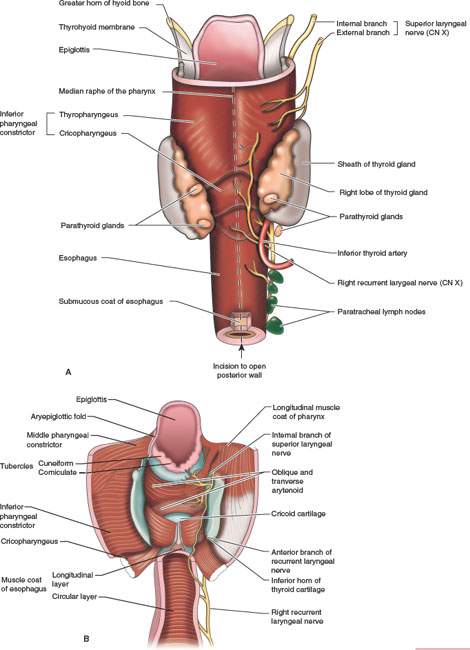
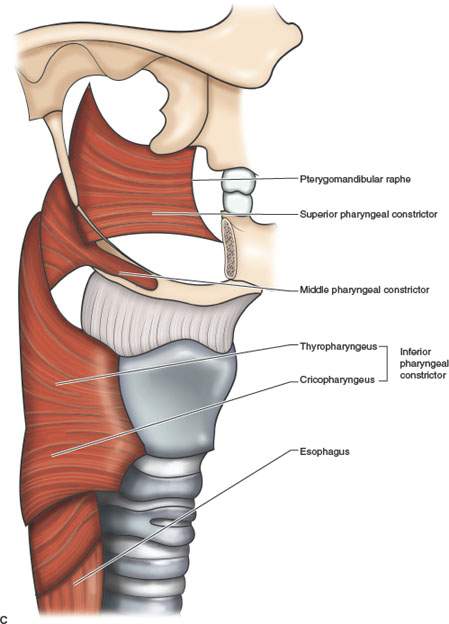
FIGURE 215.1. Views of the musculature and supporting skeleton of the hypopharynx from the posterior position. A: Note the funnellike relationship of the hypopharynx to the lower oropharynx above and the esophagus below. B: The same anatomic relationships as shown in (A) with the hypopharynx and esophagus opened from the posterior position, revealing the underlying cartilage and muscular relationships. C: Diagram of the constrictor muscle relationships to the structures at various levels of the pharynx. Note that the inferior constrictor is the main contributor to the hypopharynx, and it transitions to the sphincterlike cricopharyngeal muscular zone posterior to the cricoid cartilage.
The epithelium of the oropharyngeal and hypopharyngeal mucosa is squamous. It is continuous above with the mucosa of the nasopharynx with no visible line of transition (Fig. 215.1). There are thin constrictor muscles beneath the mucosa of the posterior and lateral pharyngeal walls. The retropharyngeal space lies between the constrictor muscles and the prevertebral fascia that covers the prevertebral muscles. That space contains a thin layer of loose fibrofatty tissue so that the entire pharynx can distend and move freely during swallowing. The constrictor muscles are thin. Beyond that inherent weakness as a barrier, there is an even more potential weak spot in the lateral pharyngeal wall just below the hyoid bone level where the middle and inferior constrictor muscles do not overlap. The lateral wall in this area is composed of the thin, fibrous thyrohyoid membrane that is penetrated by the vessels, nerves, and lymphatics of the larynx and hypopharynx; this is discussed in more detail in Chapter 201 (Fig. 215.2A,H).
The hypopharyngeal walls are continuous with the cervical esophagus below (Figs. 215.1 and 215.2). The transition to the cervical esophagus is below the arytenoids and about 3 to 4 cm in length (Figs. 215.2A,E–F; 215.3; and 215.4). This is the postcricoid portion of the hypopharynx. The lower 1 to 2 cm of this is often referred to as the cricopharyngeus muscle (Figs. 215.1, 215.2A,E–F; 215.3; and 215.4). Like the Passavant ridge, this is really only a specialized sphincterlike area of the inferior as opposed to the superior constrictor, and the “cricopharyngeus muscle” is not really a separate muscle. It is a functional zone of the inferior constrictor.
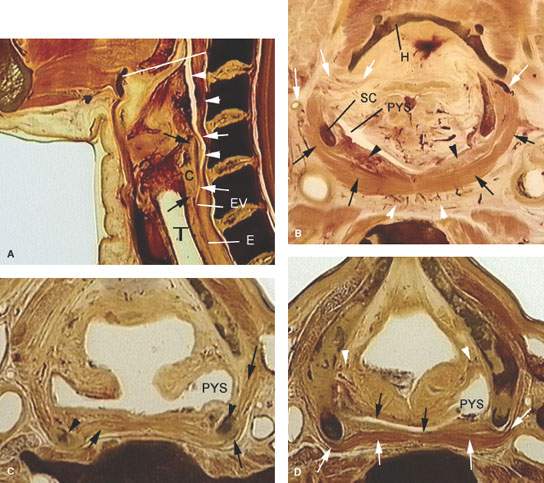
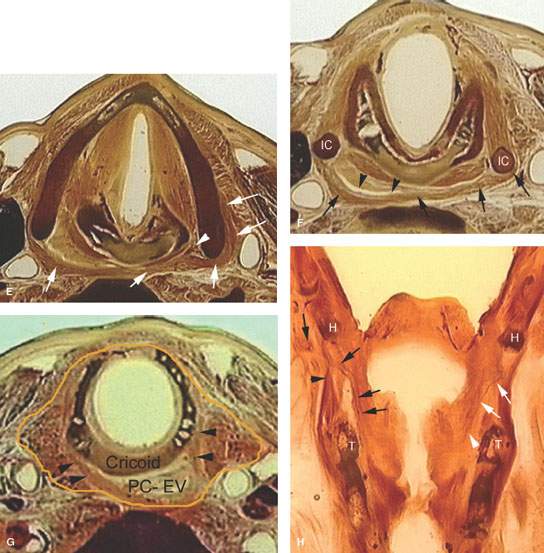
FIGURE 215.2. A series of whole organ sections demonstrating anatomic relationships of the hypopharynx. A: Sagittal section showing the cricoid cartilage (C) as a major landmark in the hypopharynx. The top and bottom of the cricoid cartilage are shown by the black arrows. The postcricoid portion of the hypopharynx is shown by the white arrows; this is one component of the hypopharynx. Above the upper level of the postcricoid hypopharynx, the other two components are the pyriform sinuses (not shown here) and the posterior pharyngeal wall and related pharyngeal lumen (white arrowheads). The white arrows show the limits of the lumen of the postcricoid portion of the hypopharynx. At the bottom of the cricoid cartilage, the esophageal verge (EV) merges with the cervical esophagus (E). (T, trachea.) Note how the hypopharynx begins at the level of the vallecula and hyoid bone (white line). B: A section through the upper hypopharynx. The hyoid bone (H) marks this level anteriorly, and the superior cornu of the thyroid cartilage (SC) is a point of attachment of the overlapping superior and middle constrictor muscles as they form the muscular posterior pharyngeal wall at this level (black arrows). Branches of the superior laryngeal vessels penetrate defects in the pharyngeal constructor muscles to enter the hypopharynx and larynx at this level (white arrows). The mucosa and submucosa of the posterior pharyngeal wall (black arrowheads) is typically not as thick as shown here but does have inherent vascularity as demonstrated. Note also the small plexus of vessels in the retropharyngeal space (white arrowheads). C: Section through the mid pyriform sinus (PYS) showing the attachment of the inferior constrictor muscle (black arrows) to the superior cornua (black arrowheads) of the thyroid cartilage. Note that the pyriform sinus has an anterior lateral and posterior wall. D: Whole organ section through the lower third of the pyriform sinus (PYS) but above the apex. Note the attachments of the inferior constrictor (white arrows) to the thyroid cartilage. The lumen of the hypopharynx along the posterior pharyngeal wall is shown by black arrows. Small branches of superior laryngeal vessels lie at the junction of the pyriform sinus and larynx deep soft tissue planes (white arrowheads). E: Whole organ section at the level of the true vocal cords to demonstrate the position of the pyriform sinus apex (white arrowhead). Note that it is adjacent to the cricoarytenoid joint. Also note the thickness of the inferior constrictor muscle as it forms the posterior pharyngeal wall and attaches to the thyroid cartilages (white arrows) at this level. This demonstrates the typical arrangement of the postcricoid portion of the hypopharynx. It is a flattened ellipsoid lying behind the cricoid cartilage. F: The inferior constrictor muscle (black arrows) attach to the inferior cornua (IC) of the thyroid cartilage. The lumen of the hypopharynx is shown by black arrowheads. G: The orange line shows the extent of visceral fascia at this level. The inferior margin of the cricoid cartilage marks the transition of the postcricoid portion of the hypopharynx to the esophageal verge (PC-EV). Note that the inferior constrictor muscles still retain an attachment to the laryngeal skeleton at this level (black arrowheads). Understanding this anatomy and its transition to the cervical esophagus is essential knowledge for proper treatment planning in hypopharyngeal and cervical esophageal cancer. H: Coronal whole organ section. This demonstrates the relationship of the pharyngeal muscular attachments to the laryngeal skeleton and penetrating neurovascular bundles. There is a gap between the hyoid bone (H) and thyroid cartilage (T). This is filled partly by constrictor muscles and infrahyoid strap muscles (black arrowhead). Note how branches of the superior laryngeal neurovascular bundle penetrate this gap (black arrows). On the opposite side, note how these vessels extend into the paraglottic space (arrowhead) and the space adjacent to the hypopharynx (white arrows).
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Cervicothoracic Junction: Brachial Plexus Trauma
Cervicothoracic Junction: Brachial Plexus Trauma
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


