Fig. 13.1
Near-infrared imaging system. PhotoDynamic Eye has a single monochrome charge-coupled device (CCD) and outputs grayscale images (a). HyperEye Medical System has a single CCD which has red, green, blue, and infrared filter on it and could output grayscale and color + infrared images (b)
PDE irradiate near-infrared (NIR) wavelength of 760 nm by using red light-emitting diode (LED) and band pass filter and observe the emission peak at the wavelength of 830 nm through long wave pass filter and a single monochrome charge-coupled device (CCD) with high sensitivity in NIR waves.
HEMS also irradiate NIR wavelength of 760 nm and observe the wavelength of 830 nm as well as the PDE. Different from the PDE, HEMS is installed single special CCD image sensor which has red, green, blue filter and also infrared filter on it and enables to detect both visible and NIR radiation simultaneously and outputs real-time color and NIR imaging.
Technique of ICG Injection
There are two ways to perform ICG injection: counter perfusion method and direct perfusion method.
Counter Perfusion Method
Counter perfusion method is based on the Glissonian approach. Procedure of counter perfusion method is as follows: Firstly, Glissonian sheath is dissected from liver parenchyma toward the tumor-bearing Glissonian pedicle from the Hilar plate and encircle the Glissonian pedicle (Fig. 13.2a). Next, ligation or tourniquet is placed and blood inflow of the planned resection area is clamped (Fig. 13.2b). Inflow occluded area becomes ischemic but unclear (Fig. 13.2c). Then ICG is intravenously injected. Observation of NIRF imaging is started about 20 s after ICG injection. Blood perfusion area, namely remnant hepatic segment, gradually generates fluorescence of ICG. On the other hand, blood nonperfusion area, namely planned resection segment, does not show the fluorescence at all (Fig. 13.2d).
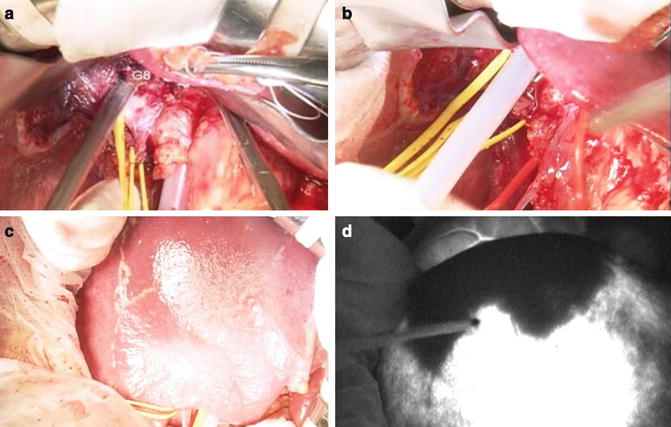
Fig. 13.2
A case of counter perfusion method for segment VIII resection is shown. Firstly, dissect of Glissonian branch (G8) from Hilar plate (a). Next, clamp G8 pedicle (b). Segment VIII become ischemic but not so clearly visible (c). After peripheral venous injection of 1 ml ICG water solution (2.5 mg/mL), segment VIII was clearly depicted by NIRF imaging (d)
Direct Perfusion Method
Direct perfusion method is the same way as the indigo carmine dye staining method. If a targeted Glissonian pedicle is far from the Hilar plate and technically the counter perfusion method is difficult, this procedure is applied. Procedure is as follows: Puncture with 23- or 21-gauge needle directly the target Glissonian pedicle (precisely, the target portal vein pedicle) under IOUS guidance. In practically, we punctured about 1 cm distal from the target Glissonian pedicle to avoid straying ICG to some other Glissonian branches. Next, inject 1 ml of 5 mg/ml ICG water solution slowly. Immediately after ICG injection, perform Pringle maneuver to avoid passing ICG away from liver parenchyma. After that, observe NIRF imaging (Fig. 13.3).
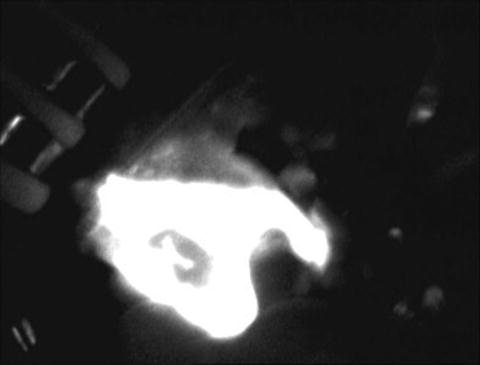
Fig. 13.3
A case of direct perfusion method for segment VI resection is shown. Immediately after direct injection of 1 ml of 5 mg/ml ICG water solution to the target portal vein, Pringle maneuver was placed to avoid passing ICG away from liver parenchyma. Fluorescence of planned resection area was maintained when Pringle maneuver was placed
Imaging Results
Images of the Counter Perfusion Method During Liver Resection
About 60 s after injection, namely in portal phase, fluorescence had maximum intensity in the remnant liver area and clearly depicted the planned resection area. Compared with macroscopic viewing, the border line was obvious. Moreover, the intensity of fluorescence was maintained during surgery (Fig. 13.2c, d).
A movie of right anterior sectionectomy using this counter perfusion method is shown (Video 13.1). After preparation of the Pringle maneuver and the Glissonian approach, the Glissonian pedicle of segment V + VIII was encircled and clamped all the time during surgery. And then 1 ml of 2.5 mg/ml ICG water solution was injected from peripheral vein. After ICG injection, NIRF image was observed. In this case, HEMS camera was used for capturing NIRF image. About 60 s after injection, fluorescence had maximum intensity in the remnant liver area and clearly depicted the planned resection area. Based on this fluorescent borderline, liver resection was performed. During liver resection, NIRF image was observed repeatedly and resection line or transection plane could be visually checked. By observing uniform fluorescence on the cut surface, we could confirm the resection was carried out as planned (Fig. 13.4a). If the resection was not carried out as planned, the cut surface does not show the fluorescence (Fig. 13.4b).
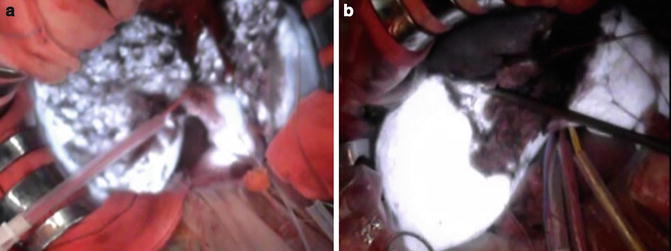
Fig. 13.4
If the dissection is carried out as planned, the fluorescence can be observed on the cut surface (a). If not, the cut surface will not show the fluorescence (b)
Images of the Direct Staining Method During Liver Resection
A movie of segmentectomy VI using direct perfusion method is shown (Video 13.2). Immediately after injection, segment VI had strong fluorescence. As blood inflow was occulted by Pringle maneuver, ICG remained at segment VI and was maintained fluorescence during the Pringle maneuver. Under this situation, the segment with fluorescence was resected.
Comments
In this chapter, the usefulness of NIRF imaging with ICG for visualizing hepatic segment during hepatectomy was presented. Liver anatomy that divides the hepatic parenchyma into Segment I to VIII based on the branching form of Glissonian pedicle has been familiar worldwide and which is recognized as the Couinaud’s segmentation. Using this Couinaud’s segmentation, current liver surgeons express the tumor-existent area and proposed anatomical resection.
In order to identify the hepatic segment during surgery, counter perfusion and direct perfusion methods were proposed as novel and useful techniques. In order to select which method is better, preoperative surgical simulation is important. Recently, three-dimensional liver anatomy reconstructed by contrast-enhanced multi-detector row CT images has been easily acquired using various applications softwares. Owing to these preoperative images, accurate intraoperative procedure could be achieved [17, 18].
Related posts:
 Intraoperative Evaluation of Regional Portal Uptake Function
Intraoperative Evaluation of Regional Portal Uptake Function
 Ureter Identification Using Methylene Blue and Fluorescein
Ureter Identification Using Methylene Blue and Fluorescein
 Near-Infrared Laser Photodynamic Therapy for Human Hepatocellular Carcinoma Cell Line Tumor with Indocyanine Green Fluorescence
Near-Infrared Laser Photodynamic Therapy for Human Hepatocellular Carcinoma Cell Line Tumor with Indocyanine Green Fluorescence
 Development of a Non-blurring, Dual-Imaging (X-Ray/Fluorescence) Tissue Marker for Localization of Gastrointestinal Tumors
Development of a Non-blurring, Dual-Imaging (X-Ray/Fluorescence) Tissue Marker for Localization of Gastrointestinal Tumors
 Fluorescein Detection of Myocardial Ischemia in an Experimental Model of Acute Coronary Occlusion
Fluorescein Detection of Myocardial Ischemia in an Experimental Model of Acute Coronary Occlusion
 Fluorophore-Conjugated Chimeric Anti-CEA Antibodies for Fluorescence-Guided Surgery of Gastrointestinal (GI) Tumors
Fluorophore-Conjugated Chimeric Anti-CEA Antibodies for Fluorescence-Guided Surgery of Gastrointestinal (GI) Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


