Fig. 14.1
24-year-old female patient presenting toxic dilation of the distal transverse colon before starting rescue medical therapy

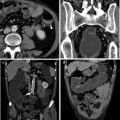
Fig. 14.2
21-year-old male presenting with acute colitis and severe bleeding (upper left). Upper right, after 36 h of intensive medical treatment the patient presented important dilation of the right colon (arrows), systemic signs of toxicity and massive bleeding. The patient underwent emergency subtotal colectomy. In the lower panel is reported the surgical specimen
Acute severe colitis accounts for the vast majority of urgent procedures and requires intensive medical treatment; this involves monitoring vital signs, treatment of electrolyte depletion, malnutrition, anaemia and toxicity, which are usually present to some degree. Specific anti-inflammatory treatment with steroids, cyclosporine or anti-TNF-α antibodies can salvage 50 % of the patients, but a high early relapse rate has been reported [8, 9]. In emergency and urgent settings portal vein thrombosis should always be assessed, since it has an incidence of 40 % and a consistent associated morbidity (see dedicated Chap. 9) [10].
Elective surgery is mainly performed for strictures, medical intractability and dysplasia or cancer. Colonic strictures have an incidence of 11 % and should be due to sub-mucosa fibrosis or mucosal hyperplasia. However, biopsies of strictures are often inadequate to role out malignancy and thus patients with long-standing disease, low-grade dysplasia in a symptomatic stricture or a stricture impassable during endoscopy have an indication to surgery. Furthermore, in the presence of a stricture a diagnosis of Crohn’s disease (CD) should always be considered for both medical and surgical therapeutic implications [8, 11]. Failure of medical management may be defined as inadequate control of symptoms with intensive medical treatment, chronic disability due to therapy and/or disease, intolerance to any pharmacological compound, medical therapy associated with excessive long-term risk (mainly steroids) and growth failure in the paediatric population [8, 9, 11–13]. Colorectal cancer (CRC) has a cumulative incidence in UC patients of 3.7 %, increasing to 5.4 % in patients with pancolitis. The cancer risk, however, increases over time and it is estimated at 2 % at 10 years, 8 % at 20 years and 18 % at 30 years of disease [14]. While an established diagnosis of CRC is an absolute indication to surgery, the management of dysplasia and dysplasia-associated lesions or masses (DALM) has to be taken with great caution. The European Crohn’s and Colitis Organization (ECCO) has published extensive practical parameters on this topic, in dedicated guidelines [15]. In fact, 42 % of patients with high-grade dysplasia and 43 % of patients with DALM may have a synchronous CRC at the time of colectomy [16].
14.3 Surgical Strategy
A number of surgical procedures are available for the treatment of UC, each with its own set of benefits and drawbacks. The surgeon, when planning surgical strategy, has to take into account several factors including patient history (in particular: preoperative medical therapy and previous surgical interventions), medical comorbidities, nutritional status and indication for surgery. The primary goal of surgery for UC is the removal of all diseased colon and rectum with the lowest morbidity and the best quality of life for every single patient. However, accomplishment of this goal may result in a winding road, and the final decision is dependent on clinical presentation (urgent or elective), anatomical characteristics, patient expectations and requires an on-going dialogue among the patient, the gastroenterologist and the surgeon.
There are four operations available for patients undergoing surgery for UC. These include conventional proctocolectomy with permanent ileostomy or Kock’s pouch continent ileostomy, abdominal colectomy with ileo-rectal anastomosis (IRA) and restorative proctocolectomy with ileal-pouch-anal anastomosis (IPAA) (Fig. 14.3).
Fig. 14.3
Surgical decision-making algorithm
Total proctocolectomy with end ileostomy has the advantage to be a single procedure that removes all disease and eliminates the risk of CRC. It is the procedure of choice for patients with impaired anal sphincter function, and distal or advanced rectal cancer. Other indications are the patient’s choice of this procedure and the presence of systemic comorbidities contraindicating a restorative procedure. Total proctocolectomy with ileostomy has a low morbidity rate, it is a definitive procedure, but more than 50 % of the patients declare to have social and psychological problems due to the presence of the stoma [9, 13, 17]. In order to reduce patient’s dissatisfaction with having a permanent stoma, Kock advocated the continent ileostomy in the 1970s [18]. In this procedure, the terminal ileum is intussuscepted within a pre-terminal ileal pouch forming a continent valve. Despite the theoretical advantages, the Kock’s pouch is performed with decreasing frequency, due to high complications rate and failure of the continence mechanism in 40–50 % of the cases [19]. IRA for UC is not a common procedure. In fact, the rationale of this intervention is based on the presence of a minimal rectal involvement, quite a rare condition in UC. Nearly 60 % of the patients initially treated with IRA ultimately failed this procedure, requiring a completion proctectomy with or without a restorative IPAA [20]. In the past decades, a new role for IRA was advocated for fertile females in order to improve fecundity, which is at high risk after IPAA due to pelvic dissection and consequent adhesions [21]. However, results from tertiary IBD centres, that perform totally laparoscopic IPAA, have shown encouraging results in terms of fecundity and delivery, making laparoscopic IPAA the procedure of choice in young women [22].
Alan Parks and John Nicholls proposed the restorative proctocolectomy with IPAA in 1978, creating “an operation that permits total removal of all disease-prone mucosa in ulcerative colitis but avoids the need for a permanent ileostomy” [23]. IPAA is a very complex procedure, based on an extended colorectal resection and an autologous transplantation to create a new rectum using the small bowel, but it is also a “quality of life” surgery. After the nineties, well past the “learning curve”, IPAA remains a highly demanding operation, with a low mortality rate in elective settings (0.2–1 %), but with a considerable morbidity. Early post-operative complication rates after IPAA vary between 28–58 %, and late complications in up to 52 %. Perioperative septic complications, related to the pouch and/or the ileo-anal anastomosis, are reported in the literature from 2.3–26.7 %. Long-term pouch failure rate ranges from 3 to 15 % [24–26]. Functional results and “quality of life” have been accessed by several studies, but with a wide variety of scores and methods and different follow-up. However, the evidence suggests that Health-Related Quality of Life (HRQoL) and Health Status (HS) of patients with ulcerative colitis improve 12 months after restorative proctocolectomy with IPAA, and are indistinguishable from the HRQoL and HS of the normal healthy population [27].
14.4 Surgical Techniques and Specific Complications
IPAA has become the preferred surgical option for the surgical treatment of UC. However, it remains a complex undertaking with the potential of remarkable short- and long-term morbidity. Successful outcomes are based upon careful patient selection, clear preoperative counselling, appropriate operative strategy and technique and adequate expertise of the surgical team in managing intraoperative problems and post-operative complications.
14.4.1 Staged Procedure
Restorative proctocolectomy may be performed as a 1-, 2- or 3-stage procedure (Fig. 14.3). A staged procedure is the procedure of choice in emergency, in acute severe colitis, when the patient is taking high dose of steroids (e.g. prednisolone >40 mg/day) or moderate steroid dose (20 mg/day) for more than 6 weeks, when differential diagnosis with CD is not established, when advanced CRC is present in the colon and in case of moderate to severe malnutrition [21]. Recent reports from Mayo Clinic and Cleveland Clinic have evidenced an increased risk of post-operative complications in patients undergoing restorative procedure under Infliximab therapy, suggesting a staged approach also for this setting [28, 29]. When appropriate skills are available, a laparoscopic approach is recommended [21]. A subtotal colectomy with end ileostomy, leaving in situ the rectum, is a relatively safe procedure even in critically ill patients, allowing patients to regain general health, normalize nutrition, interrupt any medical therapy (desaturating from steroids) and consider the option of an IPAA, an IRA or a permanent ileostomy [30, 31, 32]. There are specific recommendations on how to deal with the rectal stump, since these may have an impact on both complications and later proctectomy and IPAA. The whole rectum has to be preserved, with or without the distal part of the sigmoid colon, while dividing the rectum at the distal third is not recommended. In fact, pelvic dissection during the first procedure leads to high risk of nerves and sacral veins injury at the time of IPAA. Furthermore, post-operative pelvic fibrosis may impair ileo-anal anastomosis and jeopardize pouch function [21]. Blowout of the rectum in a very compromised bowel, due to a dehiscence of the closing suture, is the most common and dangerous complication of the staged procedure (Fig. 14.4). When necessary, a long rectal stump may allow performing a recto-cutaneous fistula, eliminating any sutured bowel from the abdominal cavity. Once again, the dehiscence of a too short rectal remnant in the pelvis should be impossible to be controlled and the consequent pelvic fibrotic reaction could lead to the impossibility of performing an IPAA.

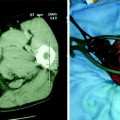
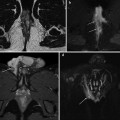
Fig. 14.4
32-year-old man in post-operative day 6 after laparoscopic total abdominal colectomy for acute colitis presenting with rectal stump dehiscence (left arrow) and visceral fluid collection (right arrow)
Proctectomy, pouch formation and ileo-anal anastomosis are the most technically demanding phases of the whole procedure. In elective cases, both resective (total proctocolectomy) and restorative (IPAA) procedures may be performed during the same intervention. Most surgeons favour creation of a temporary defunctioning loop ileostomy after IPAA to avoid anastomotic dehiscence and pelvic contamination; this is the classical two-stage procedure, since a second operation is needed, after 8–10 weeks, for ileostomy closure. However, some authors advocate the single stage procedure in selected cases, mainly on the basis of an exercise in risk management. Anastomotic dehiscence is three times higher in one-stage versus two-stage procedures (5 vs. 15 %), but ileostomy closure has the considerable complication rate of 11–25 %. So, the final decision is a balance between these two aspects, taking into account patient’s specific risk factors (e.g. preoperative therapy, nutrition, age, BMI, technical difficulties encountered during surgery) [33].
14.4.2 Pouch Configuration
Parks and Nicholls originally proposed a triple-limb S-shaped pouch, but several alternative designs have been described, including a high-capacity “W” pouch and an ease-to-perform “J” pouch [23, 34]. The evidence is that within 1 year after pouch construction, the pouch shape has no influence on functional results. However, different pouch designs have specific complications. The “S” pouch has an efferent limb that may suffer from kinking if it is longer than 1 cm, and a hand-sewn ileo-anal anastomosis with mucosectomy is necessary (see later). The “W” pouch avoids efferent limb complications, but is time-consuming with poor long-term benefits. The “J” pouch is favoured by most surgeons because of the ease of construction, allows both manual or stapled anastomosis and less intestine is used in the process [35, 36].
14.4.3 Mucosectomy Versus Double Stapling
Dissection and removal of the columnar mucosa above the dentate line with trans-anal hand-sewn anastomosis was initially advocated in order to prevent UC recurrence and CRC. The main problem with mucosectomy is due to the removal of the anal transitional zone (ATZ), which is richly innervated by sensory nerve endings that mediate anal sampling reflexes, permitting discrimination of solids and liquids from gases and thus contributing to the whole continence mechanism (Fig. 14.5) [37]. Given that when performing an IPAA the maximum length of anorectal mucosa between the dentate line and the anastomosis should not exceed 2 cm (1–1.5 cm are better), a stapled IPAA is generally preferred since it improves continence through ATZ preservation and the cancer risk is equally low as in hand-sewn anastomosis (Figs. 14.6, 14.7) [21]. Even if the advent of reliable and ergonomic stapling instruments has greatly simplified the pouch-anal anastomosis, the surgical team performing an IPAA has to be able to perform a hand-sewn anastomosis in case the stapler fails [21].

Fig. 14.5
Epithelial landmarks of the anorectal junction
Fig. 14.6
Schematic representation of a stapled IPAA. Ultra-low rectal resection is performed by a gastro-intestinal-anastomosis (GIA) stapling device (left), while the IPAA is performed by a circular end-to-end anastomosis (CEEA) stapling device (right)
Fig. 14.7
Typical aspect of an ultra-low, stapled IPAA. The vertical limbs are the staple of the rectal resection performed by the GIA (they should be vertical or horizontal, depending on the intra-operative GIA positioning), while the circular are those of the IPAA performed by the CEEA
14.4.4 Laparoscopic IPAA
In referral centres a minimally invasive approach has become the standard of care. Avoidance of wound pain and complications, reduction of blood loss and adverse surgical events, improvements of short-term and long-term morbidity, reduction of adhesion formation preserving the risk of obstruction and fecundity and a better cosmesis in a young population, are all strong points of laparoscopic surgery [22, 38–41]. Laparoscopy, together with the application of enhanced recovery programmes, designed for early post-operative mobilization and feeding, is the new gold standard of care for UC patients.
14.4.5 Sexual Dysfunction, Fecundity, Pregnancy and Delivery
Rectal and pelvic dissection may result in damage of parasympathetic erigent nerves and sympathetic hypogastric plexus, regulating ejaculation in 1–4 % of the male patients. In women, sexual dysfunction may be much higher at 8–11 %, mainly due to vaginal dryness, dyspareunia, pain interfering with sexual pleasure and limiting of sexual activity because of concerns of stool leakage [42
 Introduction
Introduction
 Surgical Perspective on Perianal Complications in Ulcerative Colitis
Surgical Perspective on Perianal Complications in Ulcerative Colitis
 Magnetic Resonance Imaging of Ulcerative Colitis
Magnetic Resonance Imaging of Ulcerative Colitis
 Water Enema Multidetector CT Colonography: Technique, Role and Imaging Findings in Ulcerative Colitis
Water Enema Multidetector CT Colonography: Technique, Role and Imaging Findings in Ulcerative Colitis
 Cross-Sectional Imaging Mimics of Ulcerative Colitis
Cross-Sectional Imaging Mimics of Ulcerative Colitis
 Imaging of Perianal Inflammatory Disorders in Ulcerative Colitis
Imaging of Perianal Inflammatory Disorders in Ulcerative Colitis




Related posts:
Introduction
Surgical Perspective on Perianal Complications in Ulcerative Colitis
Magnetic Resonance Imaging of Ulcerative Colitis
Water Enema Multidetector CT Colonography: Technique, Role and Imaging Findings in Ulcerative Colitis
Cross-Sectional Imaging Mimics of Ulcerative Colitis
Imaging of Perianal Inflammatory Disorders in Ulcerative Colitis
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
