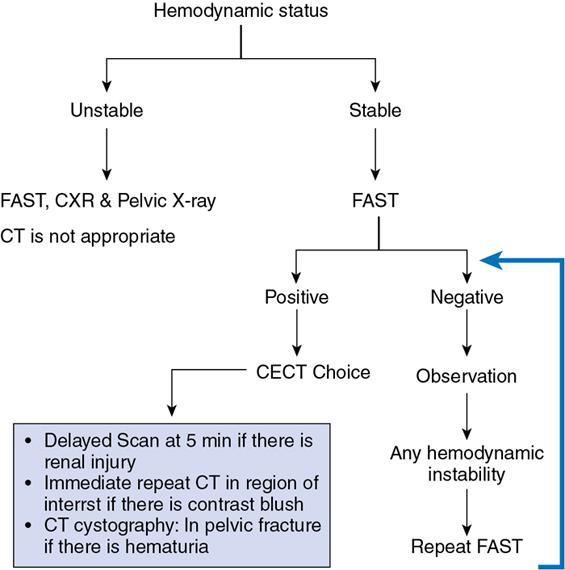
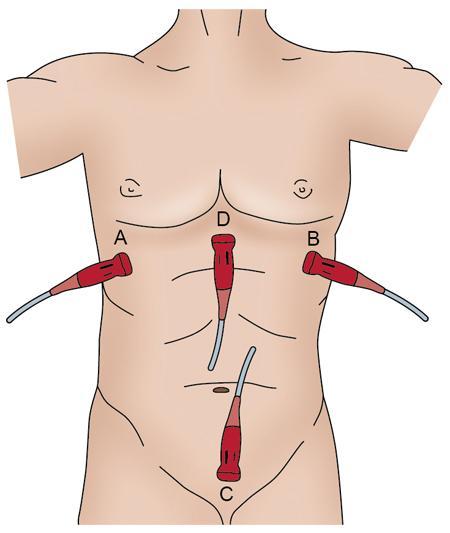
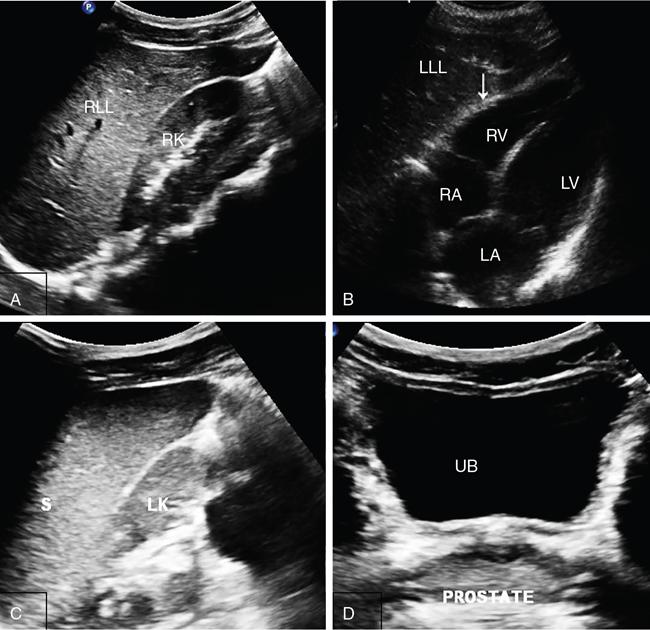
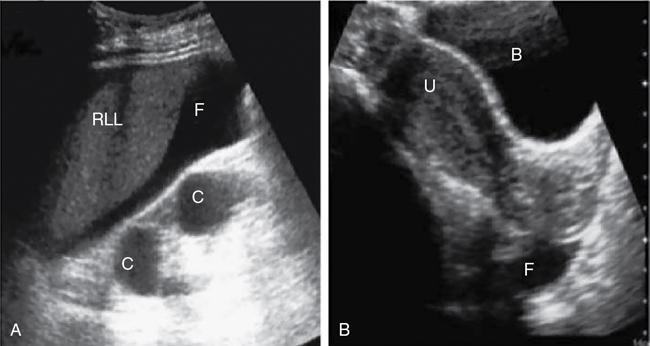
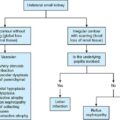
Amandeep Singh Trauma is one of the leading causes of morbidity and mortality. Blunt abdominal trauma accounts for 5% of trauma-related mortality and also contributes to 15% mortality polytrauma related mortality. More than 90% of the injuries are minor injuries and can be conservatively managed. In 10% of patients, serious injuries occur, like vascular bleeding, grade 4 or higher injuries of visceral organs, pseudoaneurysm formation, contrast or pelvicalyceal system (PCS) injury, all these require active intervention. Acute cause of death is mainly due to vascular bleed. Most common visceral organ affected in abdominal trauma is spleen followed by liver. The proper evaluation must be done of patient suffering from abdominal trauma. Abdominal trauma could be either penetrating or blunt. Blunt trauma occurs in patients of motor vehicle accidents, assault, falls and industrial accidents. Gunshot injuries and stab wounds lead to penetrating abdominal trauma. Many latest advances have been made in field of radiological imaging and imaging-guided interventional therapies, which enables nonsurgical management of haemodynamically stable patients with abdominal trauma. Contrast-enhanced computed tomography (CECT) is the investigation of choice for solid organ injures evaluation. Multidetector computed tomography (MDCT) can also help in detection of both vascular and visceral injuries following blunt abdominal trauma, for quicker examination. Thus, fast and accurate diagnosis plays a critical role in the management of patient. For appropriate care of patient imaging guideline has been recommended that includes (Fig. 7.14.1): So in haemodynamically unstable patients with blunt abdominal trauma we require: The chest X-ray erect is the earliest and most sensitive investigation for evaluation of pneumoperitoneum. With optimal radiographic technique and proper upright positioning of the patient for at least 10–15 minutes are required to detect even a small amount of air. It is possible to demonstrate up to 1.0 cc of free air on upright chest radiograph. However, plain radiographs of the abdomen are not the appropriate investigation of choice for the detection of haemoperitoneum. More than 800 cc volume of intraperitoneal blood volume is usually necessary for the demonstration of classic plain radiographic signs, for example ‘dog ear’ or ‘bladder ear’ sign when there is accumulation of intraperitoneal blood in the pouch of Douglas. Paracolic gutters are the most dependent intraperitoneal areas are where the collection of blood occurs which further displacing the right or left colon medially. The FAST is a technique for assessment of haemoperitoneum and hemopericardium (Figs. 7.14.1 and 7.14.3). It has sensitivity and specificity of more than 85% and 98%, respectively. Recently extended FAST (eFAST) protocol has come into the trauma algorithms. The eFAST examines each hemithorax for the presence of hemothorax. The FAST exam assesses the pericardial cavity and peritoneal spaces for fluid. The right upper quadrant (RUQ) evaluates the hepatorenal recess/Morrison’s pouch, the right paracolic gutter, the subdiaphragmatic area, and the caudal end of the left lobe of liver (Fig. 7.14.4a). Overall sensitivity for the detection of free fluid in the RUQ view is approximately 66%. Next is the subxiphoid (or subcostal) views to evaluate the pericardial space for any free fluid. Ultrasound detects as little as 20 cc of pericardial fluid and studies have shown excellent sensitivities and specificities approaching 100%. The subcostal view is to be required for differentiating pleural and pericardial. Left upper quadrant (LUQ) view is helpful to inspect the splenorenal recess, the subphrenic space, the left paracolic gutter and the left lower hemithorax during performing (eFAST). Similar views of the right hemithorax are obtained when scanning the RUQ. For each hemithorax view, probe has to be slide cranially above the diaphragm. The presence of the hyperechoic vertebral bodies, or ‘spine sign’, helps in identifying the fluid in the pleural cavities. US has sensitivity and specificity of 92%–100% in detection of hemothorax. Suprapubic view is beneficial in evaluating free fluid in the rectovesical pouch and cul-de-sac (rectouterine and vesicouterine) in males and females, respectively (Fig. 7.14.4b). There are no absolute contraindications to the eFAST. Curvilinear probe of frequency 2–5 MHz is used for the eFAST exam to reduce delays when switching between transducers. Likewise, the 5–12 MHz linear (or vascular) probe is ideal for assessing for pleural sliding. Although MRI does not play a role in the initial evaluation of blunt abdominal trauma. However, MRCP may be specifically useful in detecting biliary leaks. Angiographic embolization is needed when there is evidence of vascular injury (pseudoaneurysm, arteriovenous fistula) on CT scan and inactive contrast extravasation as an alternative to surgery. There is a great role of angiography in providing haemostasis in haemodynamically stable patients with high grade (IV and V) liver and spleen injuries. Computed tomography is now used as the principal imaging modality for diagnostic evaluation of abdominal trauma. It is useful in detecting both intraabdominal and retroperitoneal structure injuries and grading severity of specific parenchymal injury, along with evaluation of associated injuries of head and chest. Advantages of CT over DPL, includes detailed evaluation of injuries, associated haemorrhage and detection of any contrast extravasation. DPL has now almost become obsolete. Following a negative abdominal CT study using helical scanner, trauma patients can be discharged without a period of observation. Intravenous contrast bolus of 100–150 mL (350 mg of iodine per millilitre with total iodine load of 35–52.5 g) injected at a rate of 3–5 mL/s via 18–20 gauge cannula placed in a large peripheral vein is administered in all trauma patients. Single bolus injection method is widely used. A split bolus technique has also been proposed which has minimized the radiation exposure as a single acquisition is performed for evaluation of the abdomen. Oral contrast material for evaluating patients is no longer administered at most large trauma centres in the setting of blunt trauma. CT protocol includes portal venous phase images of the abdomen and pelvis, which are acquired at the interval of 65–80 seconds after the beginning of intravenous contrast material administration. Along with portal venous phase series, delayed phase (5–10 minutes after intravenous contrast material administration) images are necessary for patients within the amount of radiation delivered. Those with severe injury and those who have a displaced fracture of the pelvic ring, addition of an arterial phase (25–30 seconds after injection) of the abdomen and/or pelvis is required. Arterial phase helps in detection of vascular trauma that is not well appreciable on portal venous or delayed phases. With speed afforded by 64-detector scanners (and beyond), these CT angiograms can be comprehend protocols that use a single bolus of intravenous contrast material. CT cystography is done in patients suspected of bladder injury. It requires instillation of 300–400 mL of diluted water-soluble contrast material (40 mL of contrast in 360 mL of normal saline) into urinary bladder through a Foley catheter. In case of severe polytrauma, the CT cystography is done along with the delayed phase of the abdomen and pelvis which limits the radiation dose. However, it still requires full active distention of the bladder. Spleen is the most frequently injured organ following blunt abdominal trauma. Splenic injuries account for approximately 40% of all solid organ injuries occurring in abdominal trauma. Contributory factors include its potential for injury from fractured ribs, intraabdominal compression and its rich vascular supply. CECT abdomen is the modality of choice for imaging splenic injuries. Spleen shows heterogeneous enhancement on arterial phase and hence can simulate injury. So, the images should be obtained in portal venous phase. If there is dense contrast pooling seen within or around spleen, delayed CT images should be obtained to differentiate active bleeding from posttraumatic vascular injuries. Active bleeding retains the same density or even may increase in attenuation in delayed phase. Delayed phase may also be useful in differentiating a laceration from a splenic cleft. A cause of the potential inaccuracy of CT is the entity of delayed splenic rupture. Delayed splenic rupture can occur up to 48 hours after blunt trauma which should be differentiated from delayed presentation of splenic rupture due to a minor injury. On contrast-enhanced CT, splenic lacerations appear as linear low-attenuation defects within the splenic parenchyma. Shattered spleen may result due to combination of complex interconnecting lacerations. Intrasplenic haematomas appear as more diffuse hypo-attenuating regions. Splenic infarcts appear as triangular peripheral nonenhancing regions and must be distinguished from splenic haematomas. Subcapsular haematomas may occur alone or in combination with other injuries and result in low-attenuation collections that indent the splenic margin. The various CT manifestation of splenic trauma are:
7.14: Imaging and interventions in abdominal trauma
Introduction
Radiological evaluation of trauma-imaging modalities
Plain radiography
Ultrasonography
Indications for the e fast:
Contraindications
Magnetic resonance imaging
Angiography
Computed tomography
Use of contrast material
CT technique
CT signs in blunt abdominal trauma
Spleen
Choice of investigation
CT imaging findings
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


