Menstrual cycle is a dynamic balance of reproductive hormones. Imbalance of any one hormone leads to infertility.
• Follicular study or cycle monitoring is the procedure of serial ultrasonic monitoring of ovarian and uterine changes with respect to hormonal changes of menstrual cycle. This study plays an important role in fertility treatment. Hormonal changes are reflected first as Doppler changes, followed by morphological changes. It is very important to do Doppler whenever we do cycle assessment.
Role of follicular study in fertility treatment
• To assess optimal dose of drug required for stimulation of follicle.
• To assess optimal time for trigger (ovulation induction).
• To assess optimal time for oocyte retrieval in intrauterine insemination (IUI)/in vitro fertilization (IVF).
• To avoid excess stimulation and prevent ovarian hyperstimulation syndrome and multiple pregnancy.
• To reduce the rate of cycle cancellation and failure rates of IUI and IVF.
Physiology of menstruation
Basic knowledge about the normal physiology of menstruation is important to assess and interpret various grey-scale and Doppler ultrasound findings of ovarian and uterine changes in various phases of menstruation of both normal and stimulated cycles.
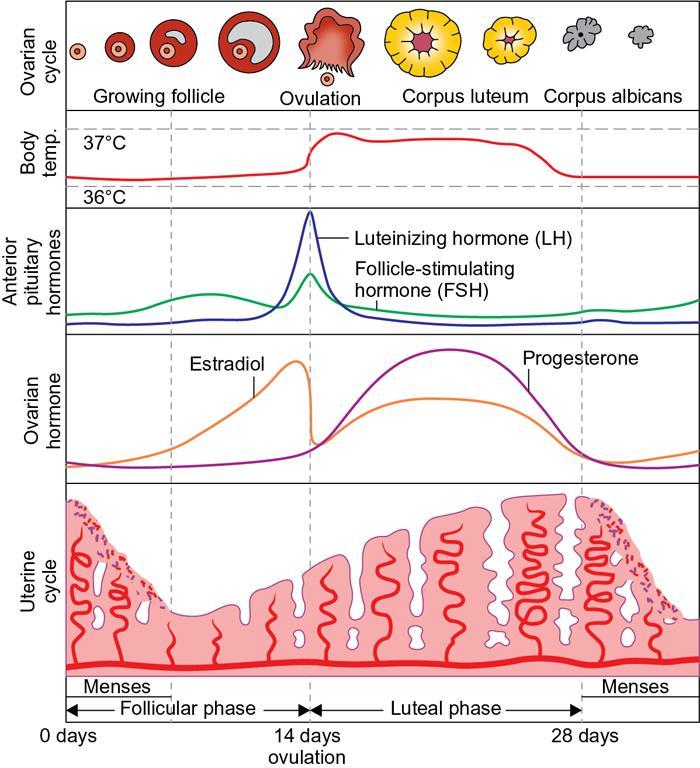
Menstrual cycle is broadly divided into proliferative and secretory phases (Fig. 11.20.1.1).
Fig. 11.20.1.1Physiology of menstruation. (Source: Slideshare.net)
Ovarian cycle
• Ovarian reserve: Four types of ovarian follicles are noted depending on the stage of development: primordial, primary, secondary and tertiary (or antral).
The true ovarian reserve is the number of primordial follicles, which is determined in the foetus and continues to decline throughout the life. Primordial follicles cannot be seen by ultrasound, as they are too small (diameter <0.05 mm).
• The fluid-filled cavity formed adjacent to the oocyte, the antrum, defines the tertiary or antral follicle. However, antral follicles are initially not identifiable by US as their diameter is less than 1 mm.
• The antral follicles are identified by US when they reach a diameter of 2 mm, correlating with higher sensitivity to follicle-stimulating hormone (FSH).
• ‘Recruitable’ antral follicles measure between 2 and 10 mm, while ‘dominant’ follicles are antral follicles >10 mm in diameter.
• Recruitment and dominance: Early recruitment (2–5 mm-sized healthy follicles forming a population) of follicle takes place in the late secretory phase of prior menstrual cycle. Second process of selection takes place during day 1–5 of the menstrual cycle. Rest of the follicles regress or become atretic.
• Process of ‘dominance’ begins on fifth to seventh day of the menstrual cycle. When a certain follicle of 10 mm size takes the control and becomes dominant which in turn suppresses the growth of the rest of the follicles. This follicle starts growing at the rate of 1–3 mm a day and reaches 17–27 mm size just prior to ovulation.
During ovulation, the dominant follicle ruptures (after luteinizing hormone [LH] surge) and releases the mature oocyte.
Corpus luteum: The ruptured follicle after getting luteinized by LH becomes corpus luteum. The corpus luteum secretes progesterone. If conception does not occur, the corpus luteum regresses and becomes corpus albicans.
Hormonal changes
FSH secreted by anterior pituitary is essential for the growth of dominant follicle and for good perifollicular flow. FSH is high in follicular phase.
LH secreted by anterior pituitary is essential for luteinization and release of oocyte from matured follicle. LH surge starts 32 h before ovulation and reaches its peak at 17 h before ovulation.
Estradiol is secreted by the dominant follicle destined for ovulation. Hence, it is minimal in the menstrual phase and shows exponential rise with the growth of matured follicle.
Progesterone is secreted by corpus luteum and correlates with the activity of corpus luteum. Hence it is absent in menstrual phase unless there is persistently active corpus luteum.
USG techniques
Transabdominal scan (TAS) is usually done once prior to transvaginal scan (TVS) to assess high placed ovaries, elongated uterus, subserosal fundal fibroids, etc.
TVS is routinely done for serial evaluation with high frequency (at least 7.5 MHz] probe.
Ultrasound settings for data acquisition especially for antral follicular count (AFC):
Transducer frequency: 7.5 MHz
Gain: −5
Enhance: 2
Speckle reduction image: 2
Reject level: 25
Harmonics: High
Follicle count may be done with either of the four techniques: real time 2D USG/2D cine loop/3D manual mode/3D sono AVC (semiautomated volume calculation).
Ultrasound techniques for counting ovarian follicles
1. Real-time 2D-US – routine standard technique
Average number of follicles in longitudinal and transverse planes is determined (Fig. 11.20.1.2).
Antral follicle size is determined by two perpendicular diameters.
• Useful to differentiate intraovarian and paraovarian structures (assessment of whether structures ‘slide’ on application of pressure by probe)
• Useful to differentiate small follicle from vessel (with application of Doppler)
• Relatively long scan time
• Does not allow offline analysis, which would be useful for training, to resolve uncertainties and for audit purposes
2. Cine-loop 2D-US – similar characteristics to real-time 2D-US
• Reduced scan time
• Allows analysis offline
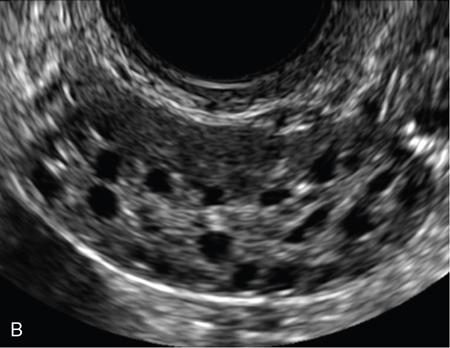
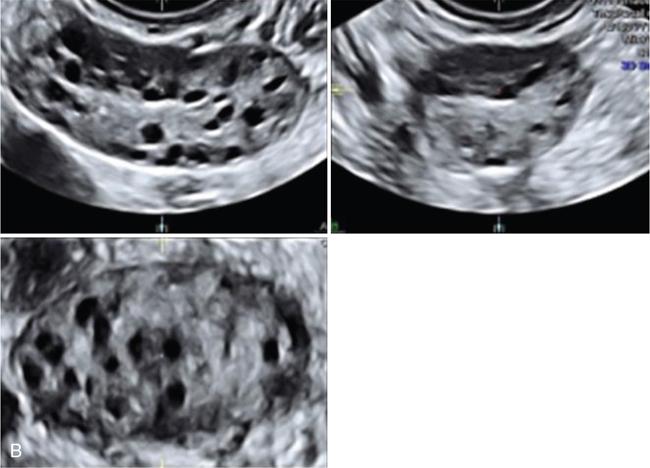
3. 3D manual mode – reproducibility is better compared with 2D methods (Fig. 11.20.1.3).
• Allowing the use of rendering mode with thin slice, on contrast enhancement, making it easier to identify follicles
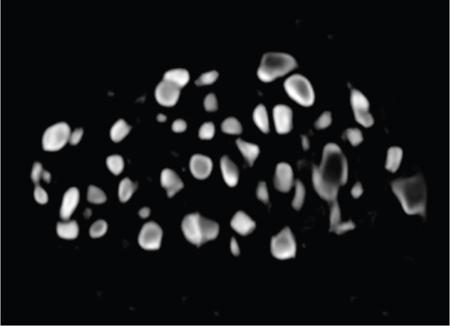
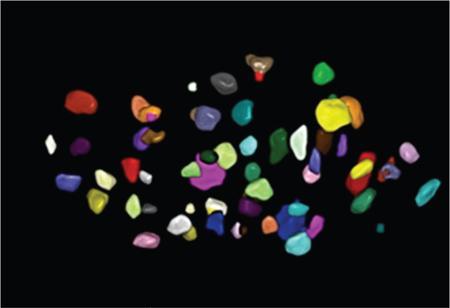
• Complete view of all follicles within volume by inversion method (Fig. 11.20.1.4).
• Special training is required with specific ultrasound systems
• They are available less widely and more expensive
• Twenty follicles are at least required for visual advantage
• Correction of problems is frequently required by manual postprocessing, for example, to include follicles which have not been identified and to exclude other extraovarian structures or tissues which are incorrectly identified as follicles (e.g. hydrosalpinx, Morgagni cysts).
• Requires specifically trained radiologists and specific ultrasound systems
• Less widely available and more expensive than standard machines
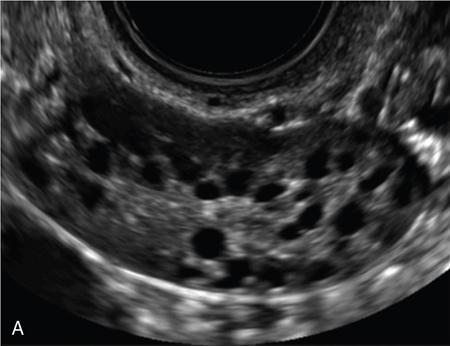
Fig. 11.20.1.2(A) Antral follicles by 2D USG without harmonics. (B) Antral follicles by 2D USG with harmonics.
Fig. 11.20.1.3(A) 3D multiplanar mode without vocal contrast imaging (VCI). (B) 3D multiplanar mode with vocal contrast imaging (VCI).
Doppler settings for cycle monitoring/follicular study
• Pulse repetition frequency (PRF) as low as 0.3
• Lowest wall motion filter
Phases of cycle assessment
• Baseline scan
• Preovulatory and ovulatory scan
• Secretory scan
Baseline Scan
Done at second to third day of the cycle
• To rule out any pelvic pathology (endometritis/polyp/adenomyosis/uterine synechiae/endometriosis, etc.)
• Look for persistent corpus luteum/anovulatory unruptured follicle
• Assess endometrial morphology and blood flow
• To assess the reserve and response
Reserve: Number of follicles that we are going to get at the end of stimulation. It depends on
1. Antral follicular count
2. Ovarian volume
Response: Means dose of gonadotropins required to produce the decided number of follicles – assessed by ovarian stromal blood flow.
TABLE 11.20.1.1
Relationship Between Total AFC and Effect of Ovarian Stimulation
Nomenclature
Total AFC
Interpretation for Ovarian Stimulation
Very low functional ovarian reserve or very small number of recruitable follicles
0–4
Very high risk of poor response to ovarian stimulation and reduced chance of pregnancy
Low functional ovarian reserve or small number of recruitable follicles
5–8
High risk of poor response to ovarian stimulation
Normal functional ovarian reserve or normal number of recruitable follicles
9–19
Expected normal response to ovarian stimulation
High functional ovarian reserve or large number of recruitable follicles
≥20
High risk of excessive ovarian response and ovarian hyperstimulation syndrome
TABLE 11.20.1.2
Relationship Between FNPO and Clinical Significance
Nomenclature
FNPO
Interpretation in Clinical Practice
Oligofollicular or low follicle count
1–3
Low ovarian reserve and increased risk of menopause in next 7 years
Normofollicular or normal follicular count
4–24
Normal follicle count for women of reproductive age
Multifollicular or high follicle count
≥25
High risk of hyperandrogenism
Antral follicle count
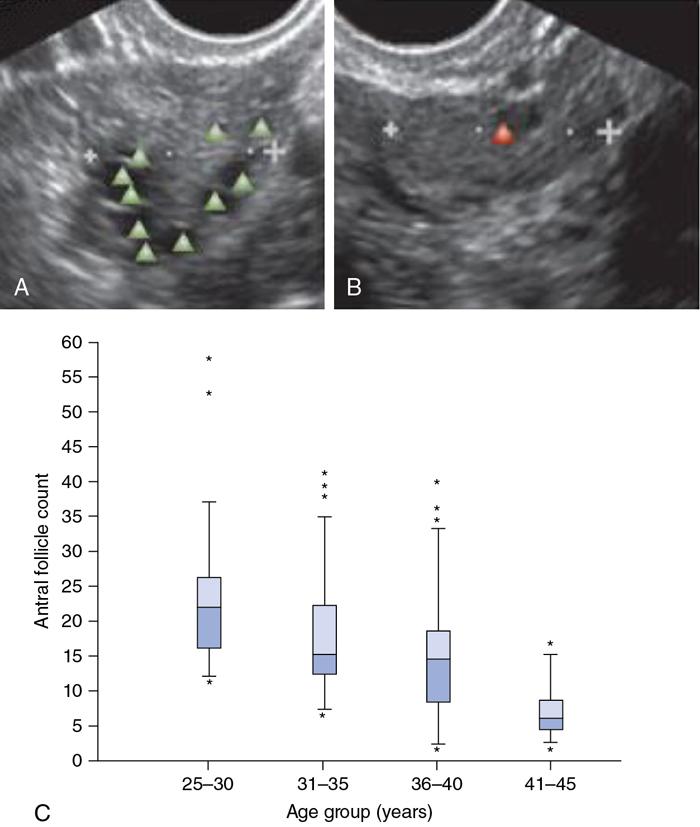
• Ovarian antral follicle count (AFC) is a noninvasive, easily performed technique that can be used as a surrogate marker for the reserve of each ovary separately (Fig. 11.20.1.6).
• AFC is preferentially done in the early follicular phase of the menstrual cycle to minimize the effect of intracycle variation (of follicular diameters) and reduces the likelihood of the presence of an ovarian cyst or a corpus luteum, which might mask some antral follicles
• Size of antral follicle – 2 to 10 mm
• Total AFC – Total number of follicles seen in both ovaries – used in assisted reproduction centres.
• Total AFC – 4 to 20 – varies every month
Fig. 11.20.1.6(A) Marks the antral follicles in transverse section. (B) Measurement of ovary in longitudinal scan. (C) Relationship of AFC with respect to age group.
Follicular number per ovary (FNPO) – useful in gynaecological clinical practice.
• AFC is also useful in predicting the risk of menopause and to raise suspicion of ovulatory dysfunction secondary to hyperandrogenism and anovulation
• AFC correlates with anti-müllerian hormone (AMH) value. Ovarian antral follicles mainly produce AMH. Accuracy of AMH and AFC are similar in providing information regarding ovarian reserve and in response prediction to ovarian stimulation.
• Limitations of assessment of AMH concentration:
1. Absence of international standardization
2. Higher cost
• The greatest advantage of AFC over AMH is while assessing the functional ovarian reserve with AFC, the observer evaluates many other aspects of the ovaries (position of ovaries, ovarian lesions, etc.), fallopian tubes (e.g. presence or absence of hydrosalpinx) and uterus (e.g. endometrial polyps or submucous leiomyomas).
Ovarian volume
• Though not a good predictor of ovarian reserve, better than basal FSH assessment
• Normal – 3 to 20 cc
• Less than 3 cc – low ovarian volume
• Low ovarian volume does not always lead to anovulatory cycle
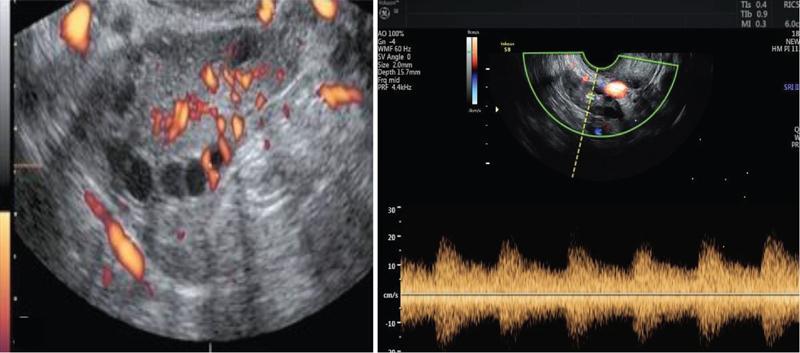
Ovarian stromal blood flow
• Ovarian stromal blood flow reflects the percentage of gonadotropins in systemic circulation that reaches the ovary
• Stromal blood flow should be assessed in the middle of ovarian stroma
• Spectral Doppler with or without 3D power Doppler study of stromal blood flow has to be done (Fig. 11.20.1.7)
• Depending on the Doppler values, the patients can be categorized as:
• Hyperresponders: RI <0.48; PSV >10 cm/s
• Normal responders: RI 0.5 to 0.7; PSV – 5 to 10 cm/s
• Poor responders: RI >0.7; PSV <5 cm/s
• In hyperresponder, the dosage of gonadotropin required for stimulation is less whereas in poor responder, the dosage required is more
• Vascularity index (VI), flow index (FI) and vascular flow index (VFI) are assessed using 3D power Doppler
• In poor responders (stromal flow index <11), recombinant LH may be added
• Stromal flow in endometriosis is less compared to normal ovary
• In polycystic ovaries with hyperinsulinism, stromal blood flow is increased due to LH and VEGF
Fig. 11.20.1.7Spectral Doppler study of ovarian stromal blood flow.
Endometrial morphology and blood flow in baseline scan
The following characteristics should be assessed:
• Intactness of endomyometrial junction
• Look for adenomyosis, polyp, submucosal fibroids
• Endometrial blood flow is a reflection of either oestrogen or progesterone
Only gold members can continue reading. Log In or Register to continue