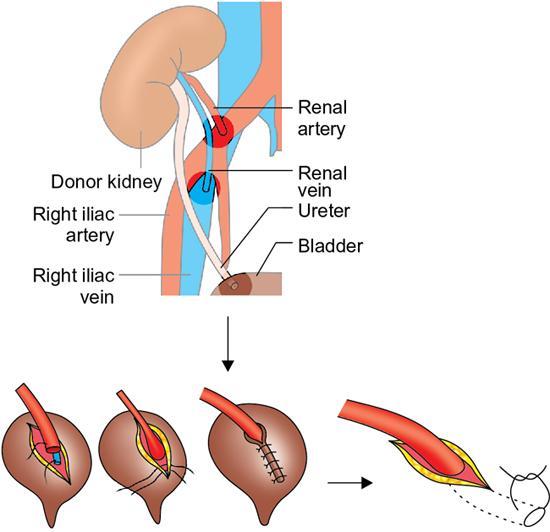
Rohan S. Valsangkar, Bhalchandra Kashyapi In renal recipient surgery, donor kidney is generally placed in the right iliac fossa extraperitoneally in adults and intraperitoneally in paediatric transplants if extraperitoneal space is small. Ureter of the donor kidney (living related or deceased donor) is anastomosed to anterolateral wall of recipient bladder by modified Lich Gregoir technique extraperitoneally (Fig. 10.19.1), while in young children or in some cases of robotic/laparoscopic renal recipient surgery, the ureter is anastomosed to the dome of bladder intraperitoneally. Care is taken to avoid redundancy of donor ureter so as to avoid subsequent kinking. The ureterovesical anastomosis is generally stented (Double J stent). Healing of anastomosis and good ureteric vascularity depends on the preservation of ureteric vascular supply by saving periureteric adventitial tissue, preservation of tissue between lower pole and ureter (golden triangle) and patency of lower polar arterial supply (if separate artery). Always seek following intraoperative details from the transplant team regarding ureteroceveisal anaestomosis: stented or not, accessory renal arteries in donor, lower polar artery anastomosis status, presence of extrarenal pelvis, borderline pelviureteric junction obstruction in the donor kidney in CT IVU (which can cause hydronephrosis post-transplant) or pre-existing small renal stones in donor kidney. Sometimes native ureter is used for anastomosis to donor ureter in inadvertent ureteric injury during retrieval. Urinary leaks occur at ureterovesical anastomotic site (technical reason/ureteral ischaemia), at proximal ureter or pelvis (inadvertent proximal ureteric or pelvis injury during donor/bench surgery). Very rarely leak can occur due to anastomosis of ureter to peritoneum, it being mistaken as bladder. Ureteric obstruction is much less common than leak and occurs in nonstented anastomosis. It is caused by oedema/clot at anastomosis. Rare causes are kinking of redundant ureter, small stone in donor kidney slipping in ureter due to diuresis.
10.19: Imaging in urological complications after renal transplantations
Surgical anatomy
Ureteral problems in early postoperative period (first 3 months)
Investigations
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine






