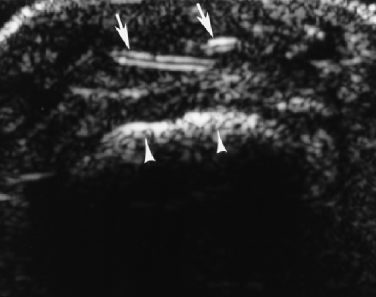
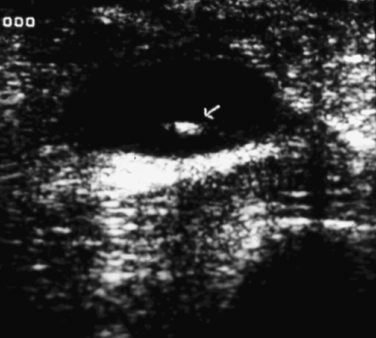
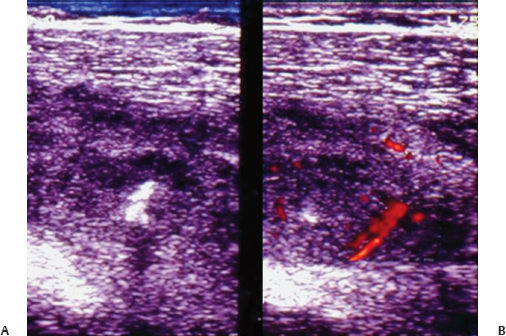
12 Imaging of Muscle, Soft Tissue, and Foreign Bodies Michael A. Bruno, Ashok Kumar Nath, A. U. Sethu, and Khamis Al Muzahmi Ultrasound is unusually well suited for the detection of foreign bodies within soft tissue. It has been shown to have greater sensitivity and specificity in the detection of a wider variety of foreign bodies than any other imaging modality, including computed tomography (CT), which is the second most-versatile method. Ultrasound has a significant advantage in that real-time imaging may also be utilized for retrieval of soft tissue foreign bodies, especially those that are not readily visualized by other methods. Nonradiopaque foreign bodies generally are quite conspicuous on ultrasound due to the striking difference between their acoustic impedance and that of the surrounding soft tissues (Figs. 12.1, 12.2, 12.3, 12.4). In addition, soft tissue foreign bodies generally are located in a superficial position, amenable to sonography. One of the first reports of the use of ultrasound for this purpose was by Fornage et al in 1986. This succinct report led to a clinical paradigm shift in the management of soft tissue foreign bodies and their conclusions were verified and extended by many other workers, notably by Little et al in 1986 and Jacobsen et al in 1998. Wood fragments, glass, plastic, and other nonradiopaque materials were shown to be easily identified on ultrasound. Currently, the preference for ultrasound for detection, identification, and localization of nonradiopaque foreign bodies is well established. In addition, the use of real-time ultrasound to guide removal of foreign bodies of all types has been well described for over a decade and indeed has become the standard of care in most major centers throughout the world (see, for example, Chapter 13). Fig. 12.1 A cactus thorn (long arrows) in the superficial soft tissues. This small foreign body would probably not be detectable by any other imaging modality. The bone cortical margin is also seen (arrowheads). (Image courtesy of Dr. M. Taljanovic, University of Arizona). Fig. 12.2 Ultrasound image of a 50-year-old male carpenter with a nonradiopaque wood foreign body in his right thigh (FB) showing as an echogenic lesion with acoustic shadowing (AC) in thigh with a draining sinus (FL) formation leading up to skin surface seen as echolucent tract. Fig. 12.3 Ultrasound of an 18-year-old village boy with history of a thorn prick and swollen calf and fever. Sonography shows an echogenic foreign body (arrow) within an echolucent abscess; the case was proven surgically. Fig. 12.14 (A) Ultrasound image of 16-year-old boy with a history of a date thorn prick in the anterior thigh showing an echogenic foreign body (FB). (B) Image shows surrounding pyomyositis with increased color flow on power Doppler. The case was proven surgically. In this chapter, we will illustrate the use of ultrasound in the diagnosis and management of soft tissue foreign bodies in the extremities, as well as the identification and management of their complications. Ultrasound also has proven utility in evaluating diseases and injuries of muscles and surrounding soft tissues; in this application there is overlap with magnetic resonance imaging (MRI), which should be considered the primary modality for the evaluation of muscle disease. We will illustrate cases where the application of ultrasound is clinically useful and decisive. Muscle, like tendons, are arranged in linear, orderly bundles called fascicles, with linear echogenic echoes oriented in parallel in the midmuscle belly, but characteristically are convergent in the distal muscle as viewed closer to the terminus tendon or aponeurosis (Fig. 12.5A). They show some degree of anisotropy to the ultrasound beam, as do tendons (see Chapters 1, 4, and 11). The most common muscle pathologies encountered in imaging are myotendinous tears and strains, contusions, and lacerations (Figs. 12.5B, 12.6, 12.7), neurogenic atrophy, infection (including abscess and pyomyositis), and inflammation (Figs. 12.8, 12.9, 12.10, 12.11, 12.12, 12.13), diabetic infarction, and necrosis. Discrete lesions such as intramuscular ganglia (cysts) are also sometimes encountered, as are occasional intramuscular lipomas and hemangiomas (Figs. 12.14, 12.15, 12.16). Malignant tumors, such as rhabdomyosarcomas, liposarcomas, and metastases are less common (Figs. 12.17, 12.18, 12.19

![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


