2 Imaging of the Elbow Gerd Gruber and Werner Konermann Translated by Axel W. E. Wismueller and Vikram S. Dogra The standard examination of the elbow joint includes the ventral and dorsal elbow joint regions. The ventral sectional planes are positioned with extended elbow, the dorsal ones with flexed elbow. For the dorsal sectional planes, using a standoff pad is recommended, as this facilitates the coupling of the transducer over the olecranon process. In the dorsal region, the elbow joint is examined in two almost perpendicular planes (transverse and longitudinal), and in the ventral region the elbow joint is examined in one transverse and two longitudinal planes. Both typical and rare pathologic findings and indications for an ultrasound examination of the elbow joint are listed in Table 2.1.
 Technique for Examination of the Elbow
Technique for Examination of the Elbow
Ventral Region: Transverse View (Humeroradial)
The ventral transverse views are obtained with the elbow joint in an extended and supinated position with the patient sitting. In patients with a significant reduction of shoulder joint motion, these views can be obtained in a supine position.
To obtain transverse views, the transducer is positioned in the distal third of the humeral shaft and then moved in a distal direction over the elbow joint. The trochlea and the capitulum humeri can be seen with their hyalin cartilage coating as a curly brace. The brachialis and brachioradialis muscles are visualized anterior to hyalin cartilage (Fig. 2.1).
Differential Diagnosis
See Figs. 2.2, 2.3, 2.4, 2.5, 2.6 for various pathologies found with a transverse view of the ventral region of the elbow.
Ventral Region: Longitudinal View (Humeroradial)
Longitudinal views of the ventral region are obtained with the elbow in an extended position. The transducer is positioned parallel to the longitudinal axes of the humeral and radial shafts. In this sectional view, the distal humeral shaft, the radial fossa, the capitulum humeri, the radial head, and the proximal radial shaft can be seen. The brachioradialis is seen anterior to the capitulum of the humerus and head of the radius. Starting at the radial head, the supinator muscle can be seen in longitudinal view anterior to the radial shaft (Fig. 2.7).
Table 2.1 Typical and Rare Pathologic Findings and Indications
| Classification | Diseases | |
| Bony changes | Cubital osteoarthritis Avascular osteonecroses and osteochondroses Free joint bodies Fracture: Fracture of coronoid process Radial head fracture | |
| Changes of bursae and joint cavity | Intraarticular volume increase (synovialis, joint efusion) Bursitis olecrani | |
| Changes of tendons and ligaments | Distal biceps tendon rupture Triceps tendon calcifcation | |
| Combined changes and other fndings | Cubital osteoarthritis (with synovitis, joint efusion) Cubital arthritis Gouty tophus Rheumatoid node Lymphadenitis Fracture Tumor | |
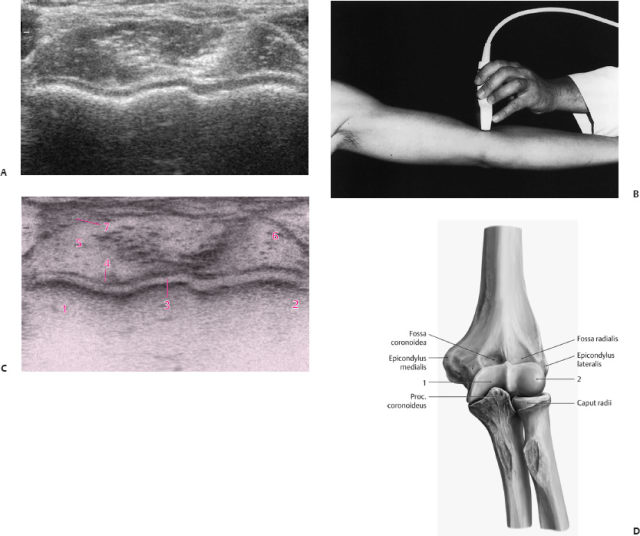
Fig. 2.1 (A) Transverse view in the distal third of the humeral shaft. (B) Transducer position. (C) Anatomic structures visualized by ultrasound, annotated in (D). (D) Anatomic position of the structures visualized in (C): 1, Trochlea humeri; 2, capitulum humeri; 3, hyalin cartilage; 4, joint capsule; 5, M. brachialis; 6, M. brachioradialis; 7, A. brachialis.
Differential Diagnosis
See Figs. 2.8, 2.9. 2.10, 2.11, 2.12 for various pathologies found with a longitudinal view of the ventral region of the elbow.
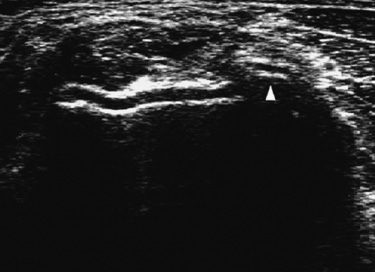
Fig. 2.2 Free joint body (arrowhead) (see Fig. 2.36C).
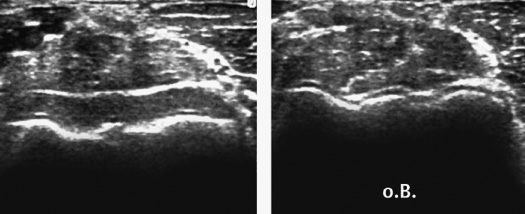
Fig. 2.3 Radial head fracture (see Fig. 2.39A).
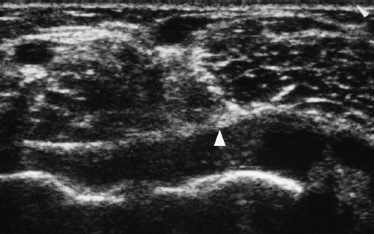
Fig. 2.4 Cubital arthritis (arrowhead) (see Fig. 2.44B).
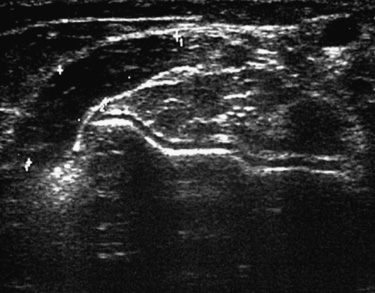
Fig. 2.5 Lymphadenitis (see Fig. 2.49A).
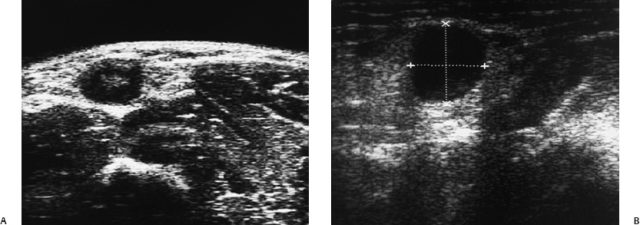
Fig. 2.6 (A,B) Tumor (see Figs. 2.50B,D).
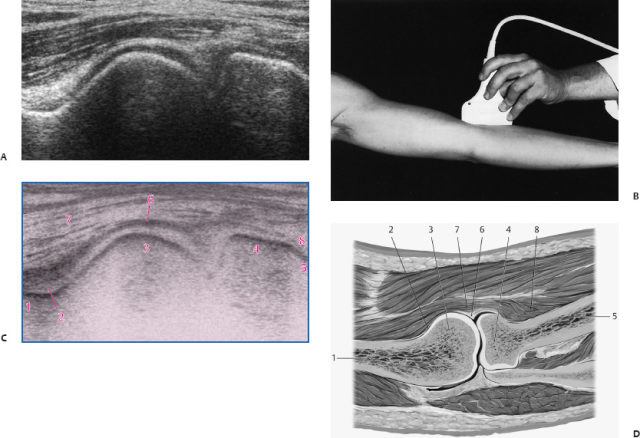
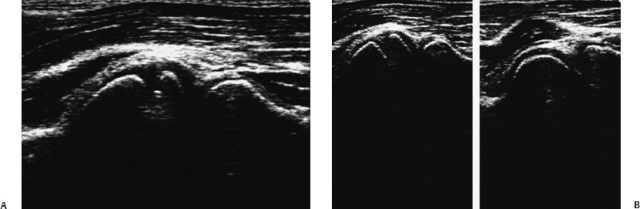
Fig. 2.8 (A,B) Osteochondrosis dissecans (see Figs. 2.35A,B).
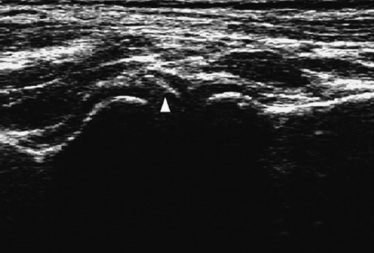
Fig. 2.9 Free joint body (arrowhead) (see Fig. 2.36A).
Ventral Region: Humeroulnar Longitudinal Section
Starting from the humeroradial longitudinal view, the transducer is moved in longitudinal axes to visualize the humerus and ulna. In this longitudinal view, the distal humeral shaft, the coronoid fossa, the humeral trochlea, the coronoid process, the proximal ulna, as well as the brachial muscle and the forearm flexors are visualized (Fig. 2.13). The humeral shaft is positioned parallel to the upper border of the screen.
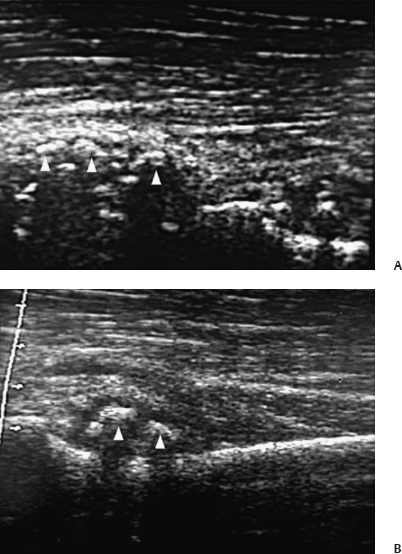
Fig. 2.10 (A,B) Chondromatosis (arrowheads) (see Figs. 2.37A,B).
Under normal conditions, the coronoid fossa appears echogenic. The positioning of the proximal ulna is frequently alleviated by a moderate flexion of the elbow joint. If extension is impaired, use of a convex transducer is recommended.
Differential Diagnosis
See Figs. 2.14, 2.15, 2.16, 2.17 for various pathologies found with a humeroulnar longitudinal view of the elbow.
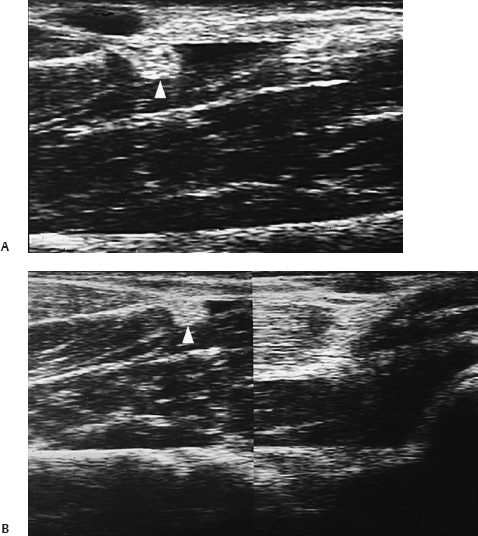
Fig. 2.11 (A,B) Distal biceps tendon rupture (arrowhead) (see Figs. 2.42A,B).
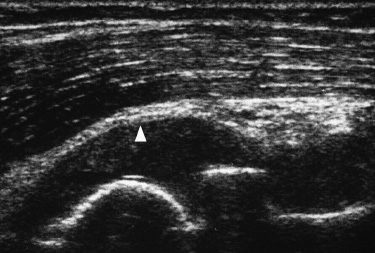
Fig. 2.12 Cubital arthritis (arrowhead) (see Fig. 2.44A).
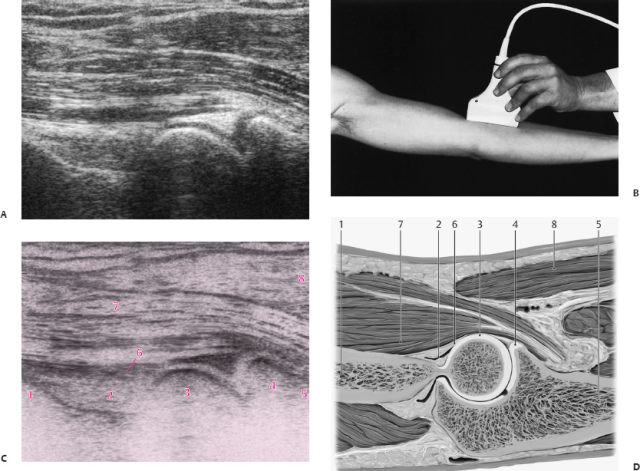
Fig. 2.13 (A) Humeroulnar longitudinal section. (B) Transducer position. (C) Anatomic structures visualized by ultrasound, annotated in (D). (D) Anatomic position of the structures visualized in (C): 1, humeral shaft; 2, fossa coronoidea; 3, trochlea humeri; 4, processus coronoideus; 5, ulnar shaft; 6, joint capsule; 7, M. brachialis; 8, forearm flexors.
Fig. 2.14 Free joint body (see Figs. 2.36B).
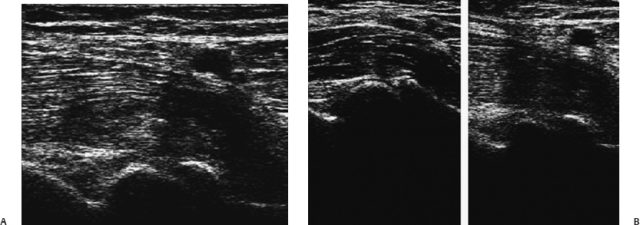
Fig. 2.15 (A,B) Fracture of the coronoid process (see Figs. 2.38A,B).
Dorsal Region: Transversal Section
The dorsal longitudinal and transverse views are obtained in a sitting position with the elbow flexed. If the patient is unable to sit, then the transducer is moved distally from the distal third so views can be obtained in supine position. The olecranon fossa forms a typical “u” shape. It is filled with fatty tissue, which appears moderately more echogenic than the triceps muscle that is running above and is imaged in a transverse view. An imaginary tangent line touching the condyles runs parallel to the upper screen edge (Fig. 2.18).
Differential Diagnosis
See Figs. 2.19, 2.20, 2.21, 2.22, 2.23, 2.24 for various pathologies found with dorsal longitudinal and transverse views of the elbow.
Fig. 2.16 Lymphadenitis (see Figs. 2.49B).
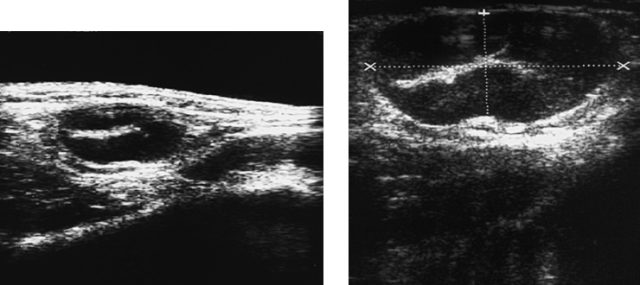
Fig. 2.17 (A,B) Tumor (see Figs. 2.50A,C).
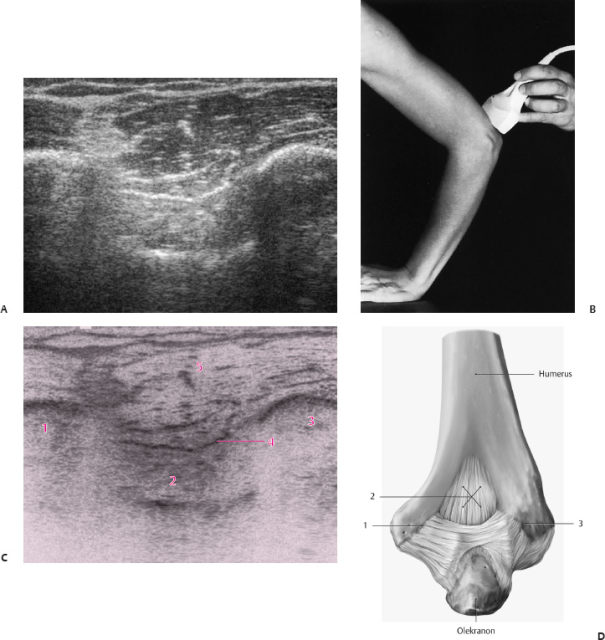
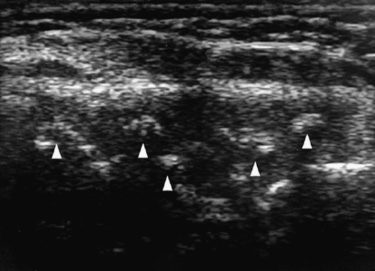
Fig. 2.19 Chondromatosis (arrowheads) (see Figs. 2.37D).
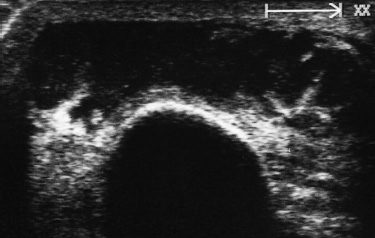
Fig. 2.20 Bursitis olecrani (see Figs. 2.40B).
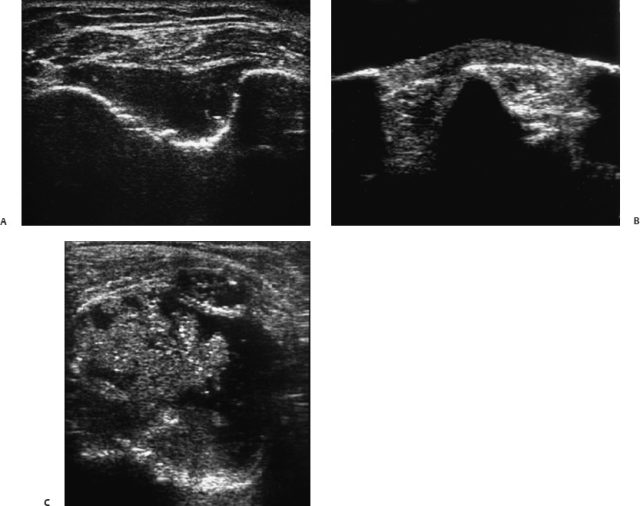
Fig. 2.21 (A,B,C) Cubital arthritis (see Figs. 2.44D, 2.45B, 2.46B).
Dorsal Region: Longitudinal Section
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


