 Clinical Indications
Clinical Indications
Trauma
Radiographs are frequently the first modality utilized in the assessment of foot and ankle trauma where most significant fractures and dislocations can be detected.
In the clinical setting, foot and ankle ultrasound is used in the assessment of ligament, tendon, and muscular injuries. An experienced operator can confidently evaluate many of the medial and lateral ligaments of the ankle, as well as the long tendons traversing the ankle joint with ultrasound. The availability of dynamic real-time evaluation of the body part also provides ultrasound with an advantage that other modalities currently do not possess.
Sometimes exposed to the perils of the surroundings, traumatic injuries to the foot and ankle may introduce foreign bodies. Radiopaque foreign bodies such as glass, gravel, or metal are detected 98% of the time with radiographs. However, ultrasound will detect nonradiopaque foreign bodies that are made of wood or plastic which radiographs will miss.
Infection
Infections of the foot and ankle are commonly seen in diabetic patients with poor podiatric care. Ultrasound can be used in the confirmation of soft tissue swelling and edema in cases of cellulitis, while concomitantly aid in the detection of abscess collections to guide drainage.
Masses
Covered with minimal soft tissue, the evaluation of masses within the foot and ankle may be performed with ultrasound. Ultrasound can provide a close-up, detailed examination of the relationship of the mass with the surrounding structures, while allowing for dynamic evaluation of the mass with respect to the neighboring tendons, muscles, and ligaments.
 Technical Guidelines
Technical Guidelines
The foot and ankle should be evaluated with ultrasound while the patient is in a relaxed position. In our practice, we frequently position the patient on either an examination bed or a reclining couch with the ankle and foot hanging over the edge. This allows for unimpeded passive and active movement of the foot and ankle during the examination.
The ultrasound probe should be a high frequency probe, preferably with a small footprint to allow for better contact with the ankle and foot surface during scanning.
 Normal Anatomy
Normal Anatomy
A systematic approach to an ultrasound study of the foot and ankle is provided below.
Lateral-Sided Ankle Structures
Structures at the lateral ankle are some of the most commonly injured. A Lauge-Hansen supination–adduction type injury frequently results in disruption of the lateral-sided ligaments.
From the anterior to posterior, the anterior talofibular, calcaneofibular, and posterior talofibular ligaments stabilize the ankle joint by holding the lateral malleolus to the talus and calcaneus.
The anterior talofibular (Fig. 6.1) and the calcaneofibular ligaments can be visualized with ultrasound (Fig. 6.2A,B). The posterior talofibular ligament is deep and overlaid by multiple structures making sonographic evaluation difficult.
The pair of peroneal tendons run and course through the lateral ankle (Fig. 6.2A,C). The peroneus brevis inserts into the lateral aspect of the base of the fifth metatarsal (Fig. 6.3); the peroneus longus inserts into the lateral margin of the plantar surface of the first cuneiform and the proximal end of the first metatarsal.
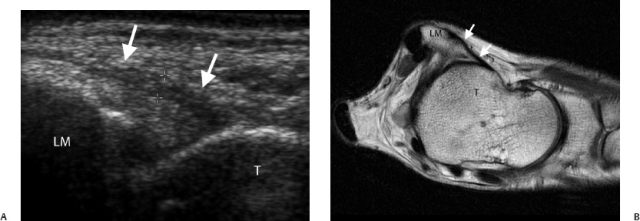
Fig. 6.1 (A) The anterior talofibular ligament (white arrows) is seen running between the lateral malleolus (LM) and the lateral aspect of the talus (T). This is best demonstrated with the ankle in a supinated and internally rotated position. (B) A comparable proton-density axial magnetic resonance image of the ankle showing the anterior talofibular ligament (white arrows) between the lateral malleolus (LM) and talus (T).
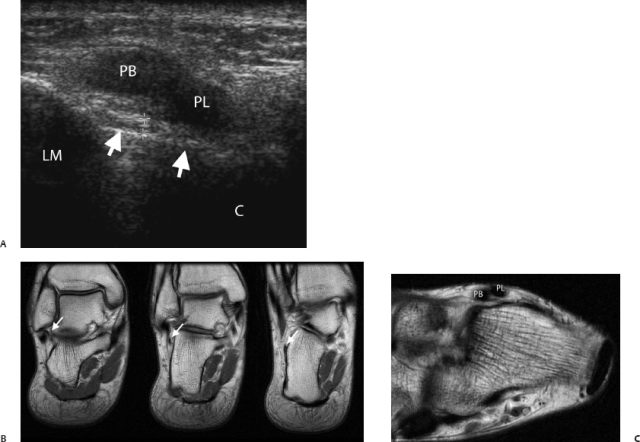
Fig. 6.2 (A) The calcaneofibular ligament (white arrows) is seen running between the lateral malleolus (LM) and the lateral aspect of the calcaneum (C). The peroneus brevis (PB) and peroneus longus (PL) tendons are seen coursing posterior and inferior to the tip of the lateral malleolus. At this position, the peroneus longus is posterior and inferior to the peroneus brevis. (B) A comparable proton density coronal magnetic resonance image (MRI) of the ankle showing the calcaneofibular ligament (white arrows). This is typically seen across several coronal images as the ligament travels in an inferoposterior direction from the lateral malleolus to the lateral surface of the calcaneum. The obliquity of this ligament should be borne in mind during sonography. (C) A comparable proton density axial MRI of the ankle rotated to match the ultrasound scanning plane showing the peroneus brevis (PB) and peroneus longus (PL) tendons in their short axis, as they course postero inferior to the lateral malleolus.
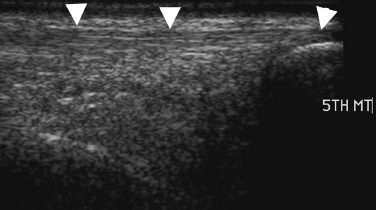
Fig. 6.3 The peroneus brevis (white arrowheads) is seen inserting into the base of the fifth metatarsal (5TH MT).
Medial-Sided Ankle Structures
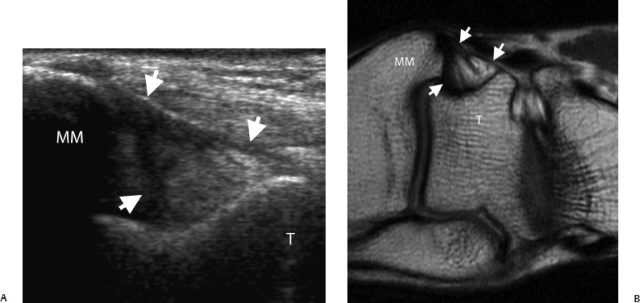
Ligaments in the medial ankle are less commonly injured. Frequently described as having superficial and deep components, the deltoid ligament is a strong ligament. The superficial component comprises the talonavicular, calcaneotibial, and posterior talotibial ligaments (Fig. 6.4). These arise from the deep surface of the medial malleolus and insert into the navicular, sustentaculum tali of the calcaneus and posterior talus, respectively. The deep component is made of only the anterior talotibial ligament.
A trio of tendons course through the tarsal tunnel in the medial ankle. From medial to lateral, they are the tibialis posterior, flexor digitorum, and flexor hallucis longus tendons (Fig. 6.5). The posterior tibial artery with its accompanying veins and the tibial nerve are also found within the tunnel (Fig. 6.6).
Anterior Ankle Structures
Three extensor tendons traverse the anterior ankle. From medial to lateral, they are the tibialis anterior, extensor hallucis, and extensor digitorum tendons (Fig. 6.7). The dorsalis pedis artery is also situated here and can be easily studied.
Posterior Ankle Structures
The stout Achilles tendon is located at the posterior ankle and is the main extensor of the foot. This conjoint tendon with contributions from both the soleus and gastrocnemius muscles inserts into the posterior surface of the calcaneus. It has a crescenteric cross-sectional profile and inserts into the posterior surface of the calcaneus (Fig. 6.8).
Plantar Structures
The plantar fascia, otherwise known as the plantar aponeurosis, runs from the medial calcaneal tubercle to the proximal phalanges of the toes (Fig. 6.9). Three components exist in this broad structure namely the medial, central, and lateral components; with the central being the most prominent.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


