 Clinical Indications
Clinical Indications
The main clinical indication for an ultrasound evaluation of the hip is the investigation of developmental dysplasia of the hip (DDH) or the follow-up of the pediatric cases with DDH. Another indication is the evaluation of the cases with hip pain, mostly having a joint effusion. The technique is also used as an adjunct to other alternative imaging modalities for the diagnosis of Legg–Calve–Perthes disease, usually presenting with the complaint of hip pain. Moreover, it is useful for the diagnosis of proximal femoral focal deficiency. It can also be used to guide percutaneous aspiration of the articular and/or extraarticular fluid collections.
 Pathologies
Pathologies
Developmental Dysplasia of the Hip
DDH includes a wide spectrum of pathologic conditions, from the stable acetabular dysplasia to irreducible dislocations. Since Hippocrates, the term congenital dysplasia was used to describe hip dysplasia and displacement in infants because it was thought to be of congenital origin. Since the 1980s, the developmental nature of the disease has been clearly understood as some infants with a normal hip examination at birth developed dysplasia of the hip during the first months after birth. Acetabular dysplasia and ligamentous laxity are the key factors in the pathophysiology of DDH.
To prevent long-term complications of the disease, an early and correct diagnosis as well as an effective treatment strategy is very important. Ultrasound is an excellent diagnostic tool for the evaluation of infants with hip dysplasia; both clinically and radiographically undetected abnormalities can be easily demonstrated by ultrasound examination alone. Graf, an Austrian pediatric orthopedic surgeon, first introduced the use of ultrasound in the diagnosis of pediatric hip dysplasia in 1980. For 30 years, it has been used to examine the hips of infants in clinical practice.
Incidence
There is no gold standard for the diagnosis of DDH in the newborn period. Both physical examination and various imaging studies, such as radiography and ultrasound, have false-positive and false-negative results. Although MRI and arthrography demonstrate the precise anatomic details of the hip, these techniques are not suitable as screening methods; instead, they are used for problem solving in selected cases. Moreover, various factors such as the age of the child at the time of the examination, genetic and racial factors, diagnostic criteria and methods, influence the incidence of DDH. Therefore, it is not possible to give a true incidence of DDH: its incidence can only be estimated. In the newborn period, the reported incidence of DDH varies from 1 to 5%. The incidence of frank dislocations is 1 to 1.5 per 1000 newborns.
Normal Sonographic Anatomy of the Hip
Knowledge of the sonographic hip anatomy is crucial for an accurate diagnosis of DDH (Fig. 7.1).
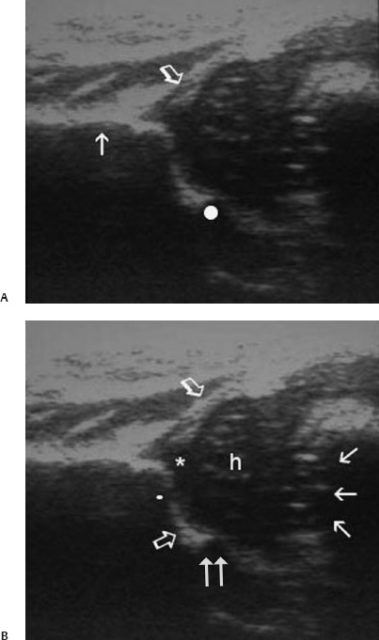
Fig. 7.1 Standard coronal plane. (A) Presence of the three landmarks, which are the lower limb of osilium (circle), midportion of the acetabular roof accompanied by straight iliac wing parallel to the horizontal plane (arrow), and labrum (open arrow) should be checked. (B) Anatomic structures to be identified adjunct to the ultrasound landmarks are the chondroosseous junction (arrows), joint capsule (oblique open arrow), head of the femur (h), hyaline cartilage roof (*), bony acetabular roof (straight open arrow), bony rim (white dot), and triradiate cartilage (double arrow) are shown.
Technical Guidelines
Ultrasound’s real-time capability allows evaluation of the dynamics of the instability as well as morphology of the hip. Soon after Graf’s initial publications about the use of hip ultrasound for the diagnosis of DDH, a different technique was developed by Novick et al and Harcke et al known as the “dynamic method” it is an imaging mimic of a clinical hip examination. Moreover, other techniques such as a modified Graf technique (Rosendahl), the Morin technique, and the modified Morin technique (Terjesen) are routinely used in the diagnosis of the hip. Whatever method is used, it is apparent that ultrasound is more sensitive than a clinical examination.
Graf’s Static Technique
Graf’s static technique is based on a morphologic evaluation of the hip in a coronal neutral view. In this technique, no emphasis is given to the position of the femoral head. The patient lies in the lateral decubitus position with the leg in neutral position slightly flexed at the hip and knee. The transducer is longitudinally oriented from a lateral approach to the hip (Fig. 7.2). Graf designed a positioning device placing the infant in the desired position, but the use of this device is optional. The highest frequency linear ultrasound probe should be used to permit an optimal penetration of the soft tissues.

Fig. 7.2 Patient is in lateral decubitus position with the leg in neutral position and the transducer oriented longitudinally.
From a technical point of view, obtaining images in the same section through the hip is crucial for a correct and reproducible ultrasound examination. Graf described a standard coronal plane for this purpose.
After subjective evaluation of the bony acetabular modeling, the bony rim, the cartilage roof triangle acetabular inclination angle (α), and the cartilage roof angle (β) are measured.
Graf classified the hips into five main groups.
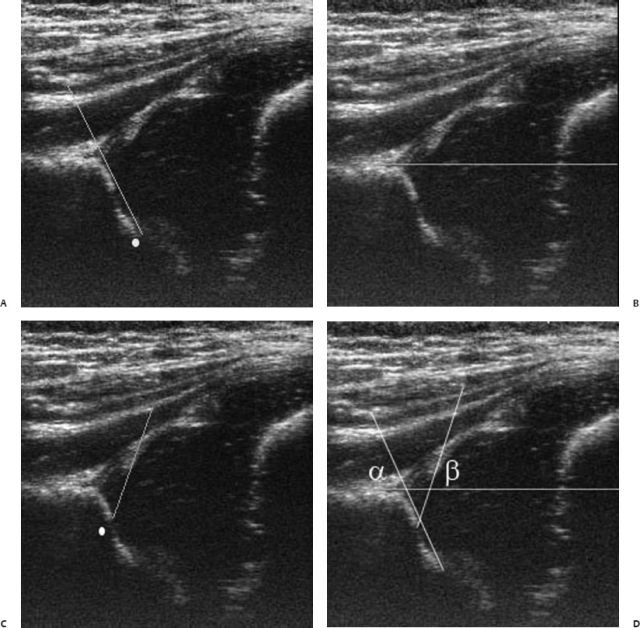
Fig. 7.3 (A) Bony roof line; tangential to the bony roof and drawn from the inferior limb of os ilium (white dot) laterally. (B) Baseline; tangential to the lateral part of the iliac wing and drawn from the uppermost part of the hyaline cartilage roof caudally. (C) Cartilaginous roof line; drawn from the bony rim (white dot) through the center of the labrum. (D)
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


