 Technical Guidelines and Normal Anatomy
Technical Guidelines and Normal Anatomy
Transducer and Equipment Capabilities
A shoulder examination is performed with a high-resolution linear array transducer. A 5 to 12 MHz and even higher frequency broad bandwidth is optimal; a lower 4 to 8 MHz frequency is useful in heavier patients. New software and hardware technologies such as tissue harmonic, compound, and extended field-of-view (FOV) imaging are essential for a technically successful shoulder examination; in fact, they have become standard techniques for musculoskeletal ultrasonography.
Patient Position
Patients are examined while seated on a revolving stool, which allows easy positioning during scanning. The examiner is seated on a wheeled chair in front of the patient.
Examination Protocol and Normal Anatomy
Shoulder sonography includes scanning the long tendon of the biceps brachialis, the rotator cuff tendon, which includes the subscapularis, infraspinatus, teres minor, and supraspinatus tendons, the glenohumeral joint, the spinoglenoid notch, and the acromioclavicular joint. The examination is completed with a series of dynamic maneuvers to assess rotator cuff impingement and glenohumeral joint fluid.
Transverse Image of the Bicipital Groove and Long Head of the Bicipital Tendon
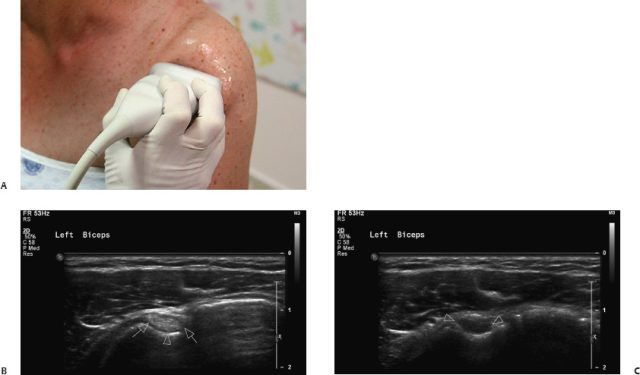
The patient is seated facing the operator; his or her hands are placed palms up on the thighs. The operator places the transducer at the humeral head (Fig. 1.1A). In an axial scan, the bicipital groove appears as a concavity in the surface of the humeral head, detected as a hyperechoic line between the greater and lesser tuberosities. The groove is an anatomic landmark to differentiate between the subscapularis tendon, which is placed medially to it, from the laterally placed supraspinatus tendon. Within the groove, the long head of the biceps tendon is seen as a hyperechoic oval structure (Fig. 1.1B). Care should be taken to avoid probe stirring that might make the tendon appear hypoechoic due to anisotropy of normal tendons (Fig. 1.1C).
Longitudinal Image of the Bicipital Groove and Long Head of the Bicipital Tendon
The whole long biceps tendon is visualized from the humeral head extending as far down as the musculotendinous junction in the humeral shaft (Fig. 1.2A). The tendon reveals a fine fibril pattern (Fig. 1.2B).
Transverse Image of the Subscapularis Tendon
The patient is asked to externally rotate his or her arm with abduction of the forearm; the transducer is turned to a transverse position and moved medially from the bicipital groove (Fig. 1.3A). The subscapularis tendon is visualized as a band of medium-level echoes (Fig. 1.3B). The subdeltoid bursa, placed over the tendon, is seen as a thin convex echogenic line. Passive internal and external rotation helps in assessing integrity of the tendon.
Longitudinal Image of the Subscapularis Tendon
The transducer is turned 90 degrees to scan perpendicularly to the tendon axis (Fig. 1.4A). The tendon is seen as several groups of fascicles in transverse orientation (Fig. 1.4B).
Transverse Image of the Infraspinatus and Teres Minor Tendons
The patient is rotated to be examined from the back, his or her hand is resting on the thigh or is elevated to the opposite shoulder (Fig. 1.5A). The infraspinatus tendon appears as a beak-shaped soft tissue structure attaching to the greater tuberosity (Fig. 1.5B). Passive external and internal rotation is useful to examine the infraspinatus tendon. By moving the transducer distal on the humerus, the teres minor may be visualized as a trapezoidal structure, differentiated from the infraspinatus by its oblique internal echoes. This small tendon may be not scanned routinely.

Fig. 1.2 Normal long head of the biceps tendon on longitudinal ultrasound view. (A) The probe is positioned over the anterior shoulder on the humeral head. (B) The tendon is seen as a fine fibril structure laterally (arrows). The collapsed subacromial-subdeltoid bursa (arrowhead) can be seen between the tendon and the overlying deltoid muscle (D).
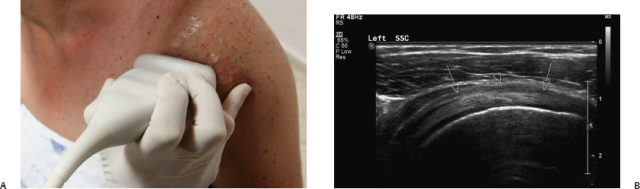
Fig. 1.3 Normal subscapularis tendon on transverse ultrasound view. (A) The probe is positioned medial to the bicipital groove for an axial scan. Note the abduction of the patient’s forearm. (B) The tendon has a convex superficial margin (arrows) and is outlined by the subacromial subdeltoid bursa (arrowhead), deep to the subdeltoid fat.
Transverse Image of the Glenohumeral Joint
The transducer is moved slightly laterally to the infraspinatus tendon (Fig. 1.6A). The articular cartilage of the humeral head is seen as a thin hypoechogenic layer adjacent to the high-level echoes originating from the bony surface. A portion of the posterior glenoid labrum is seen as a hyperechoic triangular structure (Fig. 1.6B).
Transverse Image of the Spinoglenoid Notch
The transducer is moved medially to the glenohumeral joint (Fig. 1.7A). A slightly concave bone surface is seen, which contains the suprascapular artery, and beside it, the suprascapular nerve (Fig. 1.7B). The artery may be detected as a pulsating structure on grayscale ultrasound, better detected on color Doppler.
Transverse Image of the Supraspinatus Tendon
The patient is again seated facing the operator, his or her arm adducted and externally rotated, placing the hand on the back or in the rear pocket with the palm against the body and the elbow directed posteriorly. The transducer is moved laterally from the bicipital groove, in a transverse position (Fig. 1.8A). The supraspinatus tendon is seen as a band of medium-level echoes (Fig. 1.8B). The convex echogenic line of the subdeltoid bursa is seen above the tendon. The hypoechoic layer of the articular cartilage and the bony layer of the humeral head and greater tuberosity are seen below it. The “critical zone” of the supraspinatus tendon is an area of relative avascularity, more susceptible to injury, and thus, essential to be visualized. It is located in the anterior part of the tendon, one centimeter posterolateral to the biceps tendon. The subacromial subdeltoid bursa is seen above the tendon as a very thin hypoechoic layer surrounded by hyperechoic peribursal fat. The bursa is no more than 2 mm thick including a thin internal layer of fluid.
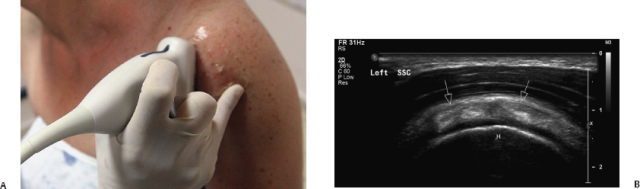
Fig. 1.4 Normal subscapularis tendon on longitudinal ultrasound view. (A) The probe is positioned medial to the bicipital groove for a sagittal scan. (B) The tendon is seen as a convex cuff of fibers (arrows) over the underlying hypoechogenic cartilage and the echogenic line of the humeral head (H).
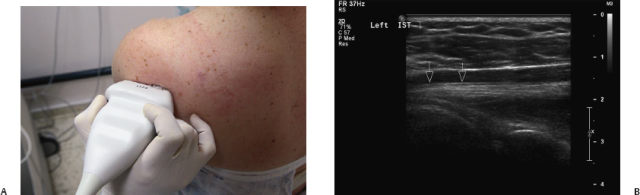

Fig. 1.6 Normal glenohumeral joint. (A) The probe is positioned slightly lateral to the infraspinatus tendon. (B) A normal rounded hyperechoic contour of the posterior humeral head (H) is seen with hypoechogenic adjacent hyaline cartilage (arrows) opposite to the glenoid ridge (G). The normal posterior glenoid labrum is seen as a triangular hyperechoic structure in the depth of the joint (arrowhead).

Fig. 1.7 Normal spinoglenoid notch. (A) The probe is positioned medial to the joint. (B) A slightly concave bone surface (arrow) is seen medial to the glenohumeral joint.

Longitudinal Image of the Supraspinatus Tendon
The transducer is turned 90 degrees to scan perpendicularly to the tendon axis (Fig. 1.9A). The tendon appears as a beak-shaped structure of medium-level echogenicity extending below the acromion to its attachment along the greater tuberosity (Fig. 1.9B).
Dynamic Maneuvers for Assessment of Rotator Cuff Impingement
The patient places his or her hand again over the thigh, palm up. The transducer is placed transversally over the acromion, the rotator cuff tendon seen below and lateral to the acromion. The patient is asked to raise his or her arm while in internal rotation, pointing the elbow up (Fig. 1.10A).

Fig. 1.9 Normal supraspinatus tendon on longitudinal ultrasound view. (A) The probe is positioned perpendicular to the tendon. (B) The “parrot-beak” appearance of the tendon (arrow) is seen in this view.
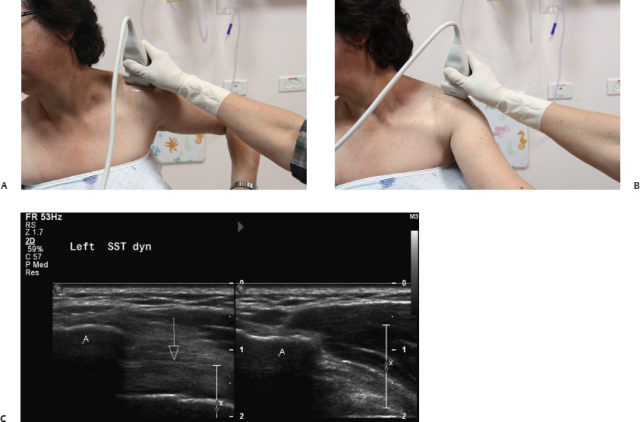
Fig. 1.10 Normal rotator cuff tendon on dynamic maneuvers. (A) The patient’s elbow is raised. (B) The patient’s arm is moved forward. (C) Left plot: the supraspinatus tendon (arrow) is seen under the acromion (A). Right plot: the tendon is hidden under the acromion (A) during a dynamic maneuver.
Afterward, the patient is asked to extend the arm with the palm facing backward and to move it forward (Fig. 1.10B). During these dynamic maneuvers, the tendon slides below the acromion being hidden by the bone acoustic shadow (Fig. 1.10C).
Transverse Image of the Acromioclavicular Joint
The patient turns his or her hand palm up on the thigh; the transducer is placed over the shoulder on a coronal plane (Fig. 1.11A). The bone echogenic lines of the clavicular distal end and the acromion are seen bridged by a hypoechoic convex structure that represents the acromioclavicular ligament (Fig. 1.11B).
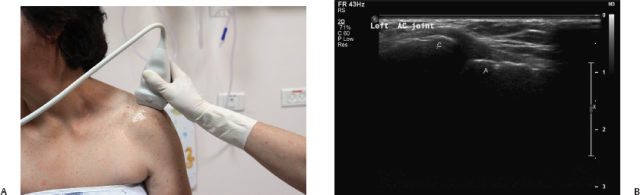
Fig. 1.11 Normal acromioclavicular joint. (A)
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


