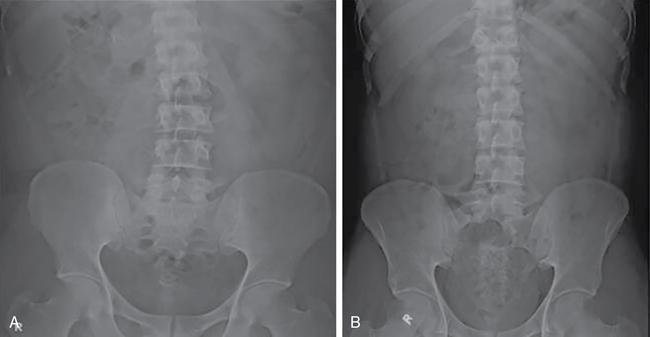
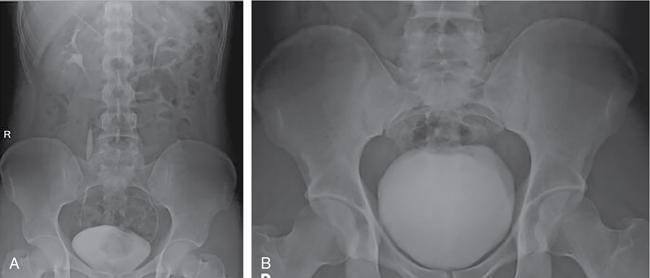
Roma Rai, Namita Singh The imaging techniques employed in an adult’s urinary system are vast with varied guidelines and algorithms. With the advent of multitude of newer imaging modalities, the strategies have constantly evolved. Non-contrast studies are still one of the strong pillars of imaging in general. However, contrast studies are an inescapable clinical necessity in majority of the cases and their usage is on a constant rise. It is therefore imperative to understand the concepts of contrast-induced nephropathy (CIN), which remains the most important possible unfavourable outcome, calling for a prudent usage of contrast. There are an array of risk factors which make a patient susceptible to the development of CIN. These risk factors are a history of diabetes mellitus, hypertension or other cardiovascular diseases, solitary kidney, renal transplant, age more than 50 years, pre-existing renal impairment, chronic infections like HIV and a patient on chemotherapy. If none of these risk factors are present, a contrast study can be performed without performing a serum creatinine. However, in presence of one or more of the risk factors, a serum creatinine followed by an estimated glomerular filtration rate (eGFR) is calculated. The patients are then stratified as very low-risk, low-risk and moderate-risk cases, using the eGFR values. In patients with eGFR of less than 60 mL/min, it is advised to consider alternative imaging modality. However, if the clinical benefits outweigh the risk of CIN, the procedure is done with precautions like withholding nephrotoxic drugs and adequate intravenous and oral hydration (pre- and post-procedure). The contrast dosage and concentration should be limited only to such an extent that the imaging quality is not compromised. The kidney ureter bladder (KUB) radiograph is the standard antero-posterior technique. The imaging is done in suspected cases of renal/ureteric colic for initial diagnosis or as a baseline for follow-up. The radiograph may rarely pick up other findings like gas in the urinary tract (emphysematous infections) or lytic bony metastases in renal cell carcinomas (Fig. 10.1.1). IVU, although replaced by CT urography in most of the centres, still remains one of the key urinary tract imaging techniques in centres having limited access to CT. IVU can be performed broadly in two ways using either the bolus infusion or the drip infusion method (Fig. 10.1.2). Bolus infusion: It is the technique widely used and it achieves better contrast opacification. The standard procedure involves patient’s preparation as that of a conventional radiograph along with a detailed history to rule out any contraindication to the contrast media in the form of a past history of allergic/anaphylactic reaction or in diabetic patients on metformin. Metformin should be discontinued in a patient for 48 hours prior to the examination. Contraindication to abdominal compression: A history of recent abdominal imaging, pain abdomen, abdominal trauma, suspicious obstruction on 5-min images or in post-renal transplant cases may lead to aggravation of the clinical condition or cause complications like urinary extravasation. Recent Advances: Digital tomosynthesis, a technique widely used in mammography, has been shown to considerably improve the adequacy of IVU. The technique is done using a standard X-ray tube and a digital flat panel detector. The tube head is rotated through an angle of 40 degrees in a horizontal direction for acquiring a set of images. The set of images acquired can be processed using different slice intervals. The literature has reported an improvement in overall adequacy to 95.5% from 46.5%, with the combined technique being pitched against computed tomography as an economically more viable option. However, the radiation dosage administered is more than the low-dosage CT technique employed in urinary calculi imaging (∼3.9 mSv). – Additional oblique views to confirm the location of visualized pathology/stone 1–3 min Delayed images till 24 hours if there is nonvisualization. ‘Rule of 6’: If there is nonvisualization of contrast in calyceal system, next film is taken after 6× interval between previous film and time of contrast given 5 min Abdominal compression applied post this acquisition 10 min (post-compression for 5 min) Collimated to kidneys Skipped in various institutions. KUB view may be added 15 min (immediately after releasing compression) Compression is not utilized routinely in many institutions Fluoroscopic visualization of contrast’s passage into the ureter followed by acquisition of the spot images Prone or supine images (gravity assisted) for opacifying post-obstructed segments Delayed images may be needed Towards the end of the procedure Oblique images for ureterovesical junction or post-void images for filling defects 98% sensitivity and 97% specificity in detecting calculous disease A non-contrast CT is adequate for calculous disease It is the imaging technique of choice in evaluating renal and urothelial malignancies Non-contrast CT can be performed even in emergency setting without any preparation Helps in detecting other possible causes of pain abdomen, e.g., appendicitis, diverticulitis, etc. Fastest technique available Provides detailed information Costlier and facility may not be available at some places Relatively less sensitive in picking up early calyceal changes Low-dose NCCT ~3 mSv Three-phase CTU-25–35 mSv Iterative reconstruction techniques have shown to reduce the dosage by half Retrograde ureterography is the technique of instilling contrast directly into the ureters by placing a catheter through bladder. The technique is seldom performed now with advent of cross-sectional imaging. It may theoretically be used as a second line of imaging to further characterise a ureteric lesion or as a primary modality in a suspected urothelial lesion having contraindication to intravenous contrast study. The practical applications are far too few in today’s imaging era. Conventional contrast techniques namely retrograde urethrography (RGU) and micturating urethrography (MCU) remains the initial imaging technique for urethra. MCU is also known as voiding cystourethrography. It is a routine to combine RGU and MCU for a comprehensive examination of urethra. Cross-sectional imaging is used for evaluating periurethral anatomy and pathology (Table 10.1.3). Ultrasound has been utilized for assessing thickness and length of urethral strictures and assessment of condition like spongiofibrosis by instilling saline.
10.1: Imaging techniques: Plain radiograph, conventional imaging, fluoro–cine techniques, USG doppler, CT/MR
Introduction
Conventional radiography
Intravenous urography
Protocol
IVU vs CTU (Tables 10.1.1–10.1.2)
Type of Image
Time from Contrast
Role
Modification
Scout KUB(patient to void bladder just before this view)
Baseline for localising the stone/other pathology
Nephrogram
Information on size, position, axis and outlines of the kidney. Indirect indicator of adequately excreting kidney
KUB
Visualization of pelvicalyceal system and ureter comparing two sides; commenting on opacification, morphology, dilatation, course of the ureter and the exact location of the calculus noted on the scout film
Kidneys
Better opacification and visualization of pelvicalyceal system
KUB
Visualization of ureter
Bladder
Only if bladder inadequately visualized on previous images
IVU
CTU
70% sensitivity and 95% specificity in detecting calculous disease and contrast administration is inescapable
Less sensitive in detecting malignancy of kidney and urinary tract
Patient preparation is essential
Information only on urinary tract
Time consuming procedure
Do not provide information on stone composition and parameters like skin to calculous distance, stone composition, etc.; factors governing surgical planning
Easily available and economical procedure
Higher spatial resolution and is therefore investigation of choice for picking up calyceal pathologies like papillary necrosis.
Mean effective dosage: 3–4 mSv
Retrograde urography
Urethrography (retrograde and micturating)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


