Fig. a–c
Normal bones (three-dimensional computed tomography reconstructions). Anterior (a), lateral (b) and posterior (c) views demonstrate the normal osseous features of the elbow; C capitellum, Co coronoid process, F olecranon fossa, L lateral epicondyle, M medial epicondyle, O olecranon, R radial head, RT radial tuberosity, T trochlea. a The arrowhead points to the sublime tubercle, and the asterisk indicates the coronoid fossa. b Arrows indicate the articular surface of capitellum
In the proximal ulna, the deep, concave trochlear notch lies between the coronoid and olecranon processes and forms a hinge joint with the trochlea. A second concave articular surface, the radial notch, lies along the lateral aspect of the coronoid process and articulates with the radial head to form the proximal radioulnar joint. The slightly concave fovea of the radial head articulates with the capitellum and the small radial tuberosity along the medial aspect of the proximal radius provides the attachment site for the tendons of the short and long heads of the biceps muscle.
The articular cartilage of the elbow is so thin that it is often difficult to evaluate with MR imaging. It is also important to recognize that the articular cartilage of the capitellum is found along its anterior convexity only, and not along its irregular, posterior nonarticular aspect. Also, the cartilage along the margins of the radial head at the proximal radioulnar joint covers approximately 60 degrees of the circumference of the radius where it articulates with the ulna at the proximal radioulnar joint.
Bones and Cartilage: MR Imaging
Most bone pathology is best identified on fat-saturated T2-weighted or STIR images [3]. T1-weighted images are useful for anatomic definition and to further evaluate abnormalities seen on T2-weighted images. For example, a fracture line is often easier to see on a T1-weighted image if the surrounding edema obscures it on a fat-saturated T2-weighted image. Articular cartilage should be evaluated in all three planes using as high a resolution technique as possible.
Bones and Cartilage: Potential Pitfalls
With the elbow extended, the border between the articular cartilage of the capitellum and its irregular nonarticular posterior surface may mimic an osteochondral lesion on coronal MR images [4]. This pitfall can be easily avoided by cross-referencing the level of the coronal scan with a sagittal image (Fig. 2). Other osseous variants that may mimic pathology involve the trochlear notch of the ulna [5]. A transverse bony ridge in the mid-trochlear notch is common and may mimic a loose body or osteophyte on sagittal images. Similarly, small cortical notches along the margins of the mid-trochlear groove may mimic osteochondral defects, again when viewed on sagittal images.
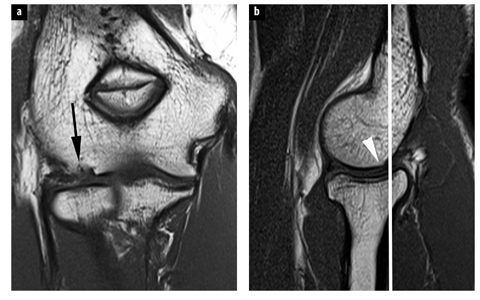
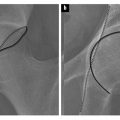
Fig. 2 a, b.
Pseudodefect of the capitellum. a Coronal T1-weighted image shows cortical irregularity along the surface of the capitellum (arrow) suggesting an osteochondral lesion. b Sagittal T1-weighted image reveals that the slice level of the coronal image (white line) is just posterior to the articular surface (arrowhead)
Bones: Pathology
Acute Trauma
In a patient presenting with elbow pain after an acute injury, often the only radiographic finding is that of an effusion (elevation of the posterior and/or anterior fat pads). Several studies have demonstrated a high incidence of associated osseous contusions or fractures in these patients that are well demonstrated with MR imaging [6–9]. A bone contusion is most easily identified by its edema-like signal intensity on fat-saturated T2- weighted images. In the case of a fracture, a linear component may be seen within the edema on T2-weighted images (Fig. 3), or may be better demonstrated as a low signal intensity line on a T1-weighted image. In the setting of a radiographically apparent fracture, MR imaging is also able to assess any associated ligament or cartilage abnormalities [10–12]. Contusions or fractures involving the radial head and posterior capitellum are commonly seen after a posterior dislocation, and should prompt close inspection of the collateral ligaments, which are often concurrently disrupted [13].
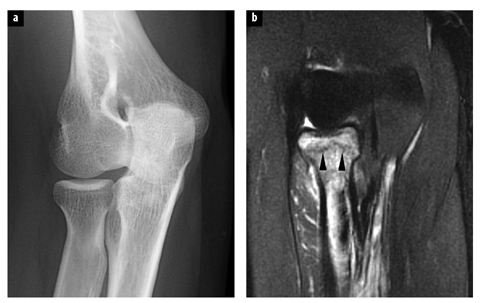
Fig. 3 a, b.
Radiographically occult fracture. a Oblique radiograph of the elbow shows no evidence of fracture. b Coronal fat-saturated T2-weighted image reveals a nondisplaced fracture of the radial head (arrowheads) with surrounding marrow edema
Osteochondral Lesions
Osteochondral lesions of the elbow are thought to result from repetitive impaction or shear forces that result in focal damage to the articular cartilage and underlying subchondral bone. Formerly known as osteochondritis dissecans, these injuries occur most often in adolescent throwing athletes or gymnasts [14].
The repetitive valgus forces that occur at the elbow during the late cocking and early acceleration phases of the throwing motion can result in tensile forces across the medial joint that may produce laxity or tearing of the ulnar collateral ligament and/or the common flexor tendon. As these medial stabilizers fail, impaction and shear forces occur across the lateral aspect of the joint resulting in injury to the cartilage and subchondral bone of the capitellum and radial head [15]. This is common in throwing athletes between the ages of 11 and 15 years (often participants of Little League Baseball) [16], and in gymnasts due to axial loading of the joint during activities involving weight-bearing on their hands.
These osteochondral lesions most commonly involve the anterolateral capitellum, but have also been described in the trochlea in young athletes. Lesions involving the medial trochlea most likely result from posteromedial abutment of the olecranon due to ligamentous laxity (see Valgus Overload Syndrome below), whereas lateral trochlear lesions are thought to result from ischemia that arises from a combination of an intrinsically tenuous trochlear blood supply and repetitive hyperextension of the elbow with posterior olecranon abutment leading to vascular compromise [17, 18].
Another mechanism for osteochondral injury of the capitellum is that of posterolateral rotary instability caused by failure of the lateral ulnar collateral ligament (LUCL), a component of the radial collateral ligament complex [19, 20]. This osteochondral lesion has been termed the „Osborne-Cotterill” lesion, named for the authors who first reported the lesion as „an osteochondral fracture in the posterolateral margin of the capitellum with or without a crater or shovel-like defect in the radial head” [21].
On MR images, post-traumatic osteochondral lesions demonstrate irregularity of the chondral surface, disruption or irregularity of the subchondral bone plate, and/or the presence of a fracture line. The primary role of imaging is to provide information regarding the stability of the osteochondral fragment, and both computed tomo-graphy (CT) and MR imaging, with and without arthrography, can provide this information to varying degrees. MR imaging, with its excellent soft-tissue contrast, allows direct visualization of the articular cartilage, as well as of the character of the interface of the osteochondral lesion with native bone (Fig. 4). The presence of joint fluid completely encircling the fragment generally indicates an unstable lesion [3, 22]. The direct injection of contrast media into the joint in conjunction with MR imaging can be helpful in two ways: (1) to facilitate the identification of intra-articular bodies, and (2) to establish communication of the bone-fragment interface with the articulation by following the route of contrast, providing even stronger evidence for an unstable fragment [23, 24]. CT arthrography can also be used for this evaluation.
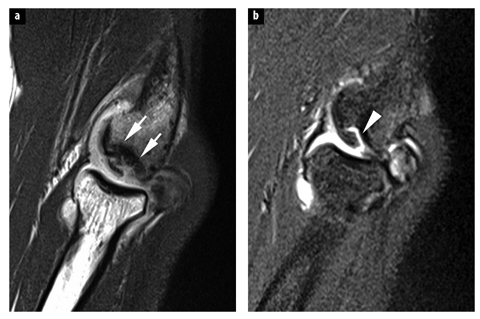
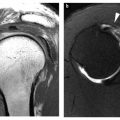
Fig. 4 a, b
Osteochondral lesion. a Sagittal T1- weighted image (magnetic resonance arthrogram) demonstrates fragmentation of the capitellum in an adolescent baseball pitcher (arrows). b Fat-saturated T2-weighted image reveals fluid partially undercutting a fragment suggesting instability (arrowhead)
Close inspection of the capitellum on coronal and sagittal MR images is important in order to distinguish a true osteochondral lesion from the normal surface irregularity produced by the pseudodefect of the capitellum described above. Additionally, the pseudodefect does not have bone marrow reactive changes or osteochondral fracture lines.
Ligaments
Ligaments: Normal Anatomy
The primary stabilizing ligaments of the elbow are found along its medial and lateral aspects (Fig. 5). The medial ulnar collateral ligament (UCL) is made up of three bundles. Its anterior bundle courses from the undersurface of the medial epicondyle to the sublime tubercle along the medial margin of the coronoid process. It is the most important stabilizer of the elbow, especially during throwing and other overhead motions. The posterior bundle of the UCL extends from the medial epicondyle in a fan-like distribution to the medial margin of the trochlear notch and forms the floor of the cubital tunnel that contains the ulnar nerve. The small transverse bundle of the UCL runs from the olecranon to the coronoid process and does not play a significant role in stabilizing the elbow [1, 3].
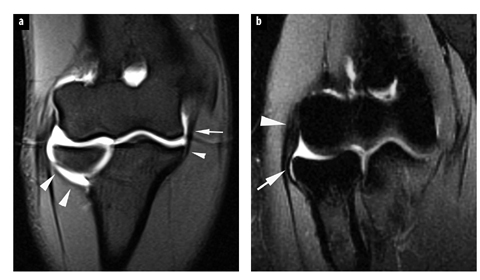
Fig. 5 a, b.
Normal ligaments. a Coronal fatsaturated T1-weighted image (magnetic resonance arthrogram) displays the anterior bundle of the ulnar collateral ligament (arrow) and its normal attachment at the sublime tubercle of the ulna (small arrowhead). Note also the lateral ulnar collateral ligament coursing posterior to the radial head to its attachment along the supinator crest of the ulna (arrowheads). b A more ventral coronal fat-saturated T1-weighted image from a magnetic resonance arthrogram shows the radial collateral ligament (arrow) just deep to the common extensor tendon (arrowhead)
On the lateral side, the radial collateral ligament lies just deep to the common extensor tendon and courses from the lateral epicondyle to blend with the annular ligament along the volar aspect of the radiocarpal joint. The LUCL also originates on the lateral epicondyle where it is inseparable from the radial collateral ligament, and extends behind the radial head to attach to the supinator crest along the lateral aspect of the proximal ulna. It provides posterolateral stability for the radiocapitellar joint [23]. The annular ligament runs from the ventral aspect of the radial notch around the radial head to attach along with the LUCL along the supinator crest of the ulna and stabilizes the proximal radioulnar joint [24]. Although these are described as individually, more recent studies suggest that these structures function together as a continuous sheet, rather than as individual entities [23, 25].
Ligaments: MR Imaging Technique
The collateral ligaments of the elbow are best evaluated on coronal and axial images and should appear as low signal intensity structures on all sequences. However, given their collagen structure, ligaments will be susceptible to magic angle artifacts on „short TE” images (T1, proton density, gradient echo).
Ligaments: Potential Pitfalls
Some degree of increased signal intensity is often present within the proximal portion of the anterior bundle of the UCL on fluid-sensitive MR imaging sequences and can mimic true pathology in this region. The anterior bundle normally may also demonstrate a striated appearance on MR imaging. The same holds true for the LUCL, and it should be noted that this ligament might not be seen in some patients on MR images (up to 15% in one study).
Ligaments: Pathology
Valgus Instability
The UCL, and in particular its anterior band, is the most important medial stabilizer of the elbow from 30 to 120 degrees of flexion. The most common mechanisms of ulnar collateral ligament insufficiency are chronic attenuation, as seen in throwers or other athletes using an over- head motion, and an acute post-traumatic disruption, usually after a fall on an outstretched arm [26]. During the throwing motion, high valgus stresses are placed on the elbow with resulting tensile forces along its medial aspect. The maximum stress on the ulnar collateral ligament occurs during the late cocking and acceleration phases of throwing [27]. Repetitive insults to the ligament produce microscopic tears that progress to significant attenuation or frank tearing within its substance. Complete, full thickness tears are often well demonstrated on conventional MR imaging studies, but partial tears can be subtle and are best seen with MR arthrography (Fig. 6) [28, 29]. While MR imaging facilitates direct visualization of the ligament complex, in chronic cases the development of heterotopic ossification along the course of the ligament has been described [30].
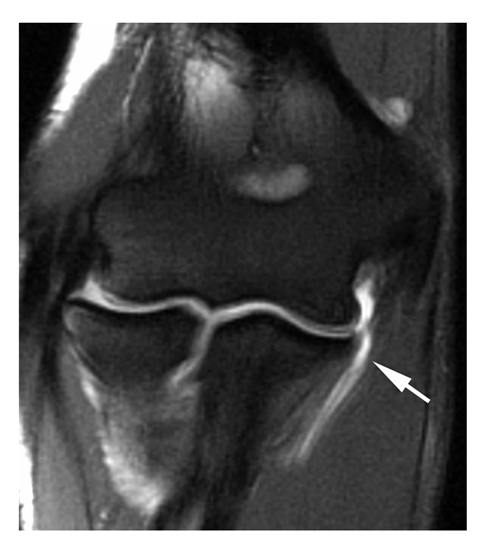
Fig. 6
Ulnar collateral ligament (UCL) tear. Coronal T2-weighted image (magnetic resonance arthrogram) demonstrates a tear of the UCL at its distal insertion (arrow) with extravasation of fluid into the adjacent soft tissues
In the skeletally immature patient, the apophysis is the weakest link in the muscle-tendon-bone complex and an acute injury may result in avulsion of the epicondyle into the joint where it may simulate an intra-articular osseous body. Ultrasound [31], CT and MR imaging can show these avulsions. Nonunion can lead to repeated valgus instability.
More commonly, chronic valgus stress may result in a condition known as „Little Leaguer’s elbow” in which stress across the physeal plate results in its apparent widening on radiographs (also known as „epiphysiolysis”) or displacement or fragmentation of the medial epicondylar apophysis [32]. MR imaging demonstrates extension of physeal cartilage into the metaphysis and/or marrow edema within the apophysis, and also allows for assessment of the UCL, which is usually normal in these patients [33] (Fig. 7).
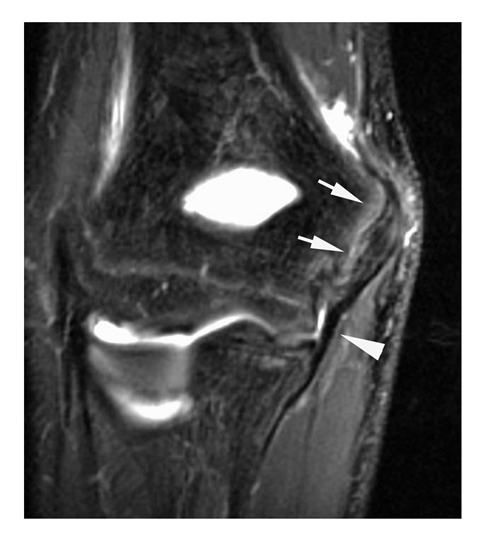
Fig. 7
Medial epicondylar epiphysiolysis („Little Leaguer’s elbow”). Coronal fat-saturated T2-weighted image (magnetic resonance arthrogram) displays marrow edema along the medial epicondylar apophysis (arrows) in a young baseball player. Note also the normal ulnar collateral ligament (arrowhead)
Valgus Overload Syndrome
Throwing athletes and others involved in overhead sports often develop a constellation of injuries known as the valgus overload syndrome [34–36]. This is related to the strong valgus forces that occur primarily during the late cocking and early acceleration phases of the throwing motion, which may lead to tensile failure of the UCL, an osteochondral lesion in the capitellum (related to lateral impaction forces) and subchondral edema, cartilage loss and/or osteophyte formation along the posteromedial trochlea secondary to increased shear forces in that region [37] (Fig. 8). Therefore, a careful inspection of these three areas should be carried out when viewing an MR imaging study in an overhead throwing athlete presenting with elbow pain, but it should be noted that imaging abnormalities at these sites are also common in asymptomatic athletes [38].
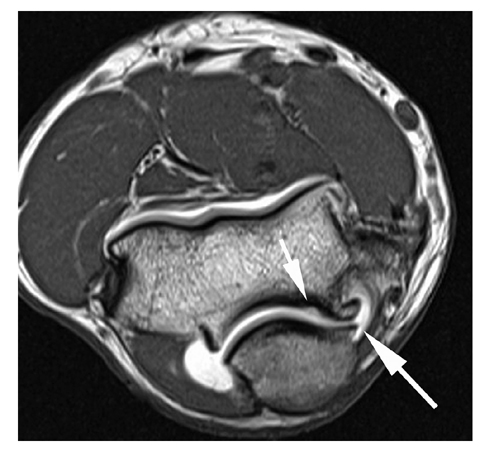
Fig. 8
Valgus overload syndrome. Axial T1-weighted image (magnetic resonance arthrogram) demonstrates prominent osteophytes along the posteromedial joint (large arrow) as well as a small focus of cartilage loss along the posterior trochlea (small arrow)
Varus Instability
Lateral elbow instability related to isolated abnormalities of the lateral collateral ligament complex is related to a stress or force applied to the medial side of the articulation, resulting in compression on that side, and tensile forces across the lateral joint producing insufficiency of the radial collateral ligament complex. This most often occurs during an acute injury, but may rarely result from repetitive stress. Other causes of varus instability include dislocation, subluxation and overly aggressive surgical technique during release of the common extensor tendon or resection of the radial head.
Posterolateral Rotary Instability and Elbow Dislocation
Posterolateral rotary instability (PLRI) is the most common pattern of recurrent elbow instability (Fig. 9). PLRI represents a spectrum of pathology consisting of three stages, according to the degree of soft-tissue disruption. In stage 1, there is posterolateral subluxation of the ulna on the humerus that results in insufficiency or tearing of the LUCL [39–41]. In stage 2, the elbow dislocates incompletely so that the coronoid is perched under the trochlea. In this stage, the radial collateral ligament and anterior and posterior portions of the capsule are disrupted, in addition to the LUCL. Finally, in stage 3, the elbow dislocates fully so that the coronoid rests behind the humerus. Stage 3 is subclassified into three further categories. In stage 3A, the anterior bundle of the medial collateral ligament is intact and the elbow is stable to valgus stress after reduction. In stage 3B, the anterior bundle of the medial collateral ligament is disrupted so that the elbow is unstable with valgus stress. In stage 3C, the entire distal humerus is stripped of soft tissues, rendering the elbow grossly unstable even when a splint or cast is applied with the elbow in a semiflexed position. This classification system is helpful, as each stage has specific clinical, radiographic and pathologic features that are predictable and have implications for treatment [40].
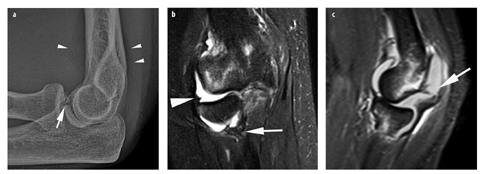
Fig. 9 a–c.
Elbow dislocation. a Lateral radiograph obtained after a fall on an outstretched arm reveals elevation of the anterior and posterior fat pads (arrowheads) as well as a nondisplaced fracture of the coronoid process (arrow). b Coronal fat-saturated T2-weighted image demonstrates lateral subluxation of the radial head, proximal disruption of the lateral ulnar collateral ligament from its humeral attachment (arrowhead), and partial tearing of the ligament at its ulnar attachment (arrow). c Sagittal STIR image reveals bone marrow contusions in the proximal radius and in the posterior capitellum, which is also slightly impacted. The posterior capsule is also disrupted (arrow)
Subluxation or dislocation of the elbow can be associated with fractures. Fracture-dislocations most commonly involve the coronoid process and radial head, a constellation of findings referred to as the „terrible triad” of the elbow, since this injury complex is difficult to treat and prone to unsatisfactory results [40].
A shear fracture of the coronoid process of the ulna is commonly seen following elbow dislocations. This fracture is pathognomonic of an episode of elbow subluxation or dislocation, and the larger the coronoid fracture fragment, the higher the degree of posterolateral instability [42]. A fracture of the radial head does not cause clinical instability. Injuries of the articular surfaces may occur during elbow subluxation, as described in the section on osteochondral lesions.
Another consideration with respect to elbow dislocation is that, as the ring of soft tissues is disrupted from its posterolateral to medial aspects, tearing of the capsule allows joint fluid to escape into the periarticular tissues and, as a result, radiographic signs of an effusion, indirect evidence of elbow trauma, might not be present.
Plicae
Plicae: Normal Anatomy and Pathology
Synovial plicae represent embryologic remnants that are commonly found within asymptomatic elbows. The most common of these synovial folds is the posterolateral plica [43] (also known as the radiohumeral plica, radiocapitellar plica or „synovial fringe”); anterior and posterior plica are less common (Fig. 10).

Fig. 10
Normal plica. Coronal fat-saturated T1-weighted image (magnetic resonance arthrogram) demonstrates a lateral radiocapitellar plica (arrow)
The posterolateral plica is present in 86% of cadavers and up to 98% of asymptomatic patients on MR imaging [43, 44]. Even so, it has been implicated as a cause of lateral elbow pain known as the „synovial fringe syndrome” [45]. This is thought to result from dynamic entrapment of the plica between the radial head and capitellum and often produces snapping, popping or even locking of the elbow [46–49]. Histologically, the plica becomes thickened and fibrotic and this may result in focal cartilage loss along the lateral aspect of the radial head. The MR imaging findings of a plica measuring greater than 3 mm in thickness or covering more than one-third of the articular surface of the radial head should raise suspicion for the diagnosis, but must be correlated with clinical findings since there is an overlap in the MR imaging appearance of the posterolateral plica in symptomatic and asymptomatic patients.
Tendons and Muscles
Tendons and Muscles: Normal Anatomy
The biceps tendon courses across the elbow anteriorly to insert on the radial tuberosity and is best seen in the axial plane (Fig. 11). The bicipital aponeurosis (lacertus fibrosus) is a fascial extension from the short head of the biceps that extends over the biceps tendon and provides some tendon stability in this region. The long and short heads of the tendon can usually be distinguished on cross-sectional imaging and should not be mistaken for a longitudinal tear near its insertion [50]. Immediately deep to the biceps lies the brachialis muscle and its very short tendon that attaches to the ventral aspect of the coronoid process of the ulna.
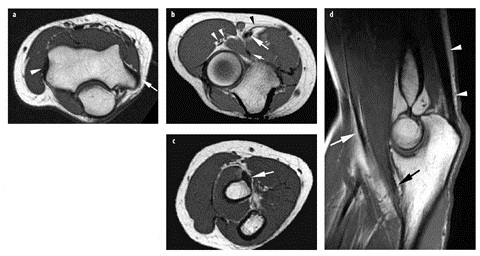
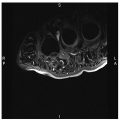
Fig. 11 a–d.
Normal tendons. Axial T1- weighted images show: a the common flexor/ pronator (arrow) and common extensor (arrowhead) tendons, b the biceps tendon (large arrow), lacertus fibrosis/bicipital aponeurosis (black arrowhead), brachialis tendon (small arrow) and branches of the radial nerve within the radial tunnel (white arrowheads), c the distal biceps tendon at its insertion on the radial tuberosity (arrow). d Sagittal T1-weighted image again demonstrates the biceps tendon (white arrow), brachialis tendon (black arrow) and triceps tendon (arrowheads)
Posteriorly, the triceps tendon attaches along the dorsal aspect of the olecranon, distal to its tip. The small anconeus muscle lies along the posterolateral aspect of the elbow, arising from the posterior aspect of the lateral epicondyle and inserting along the proximal ulna.
The flexor/pronator muscles of the forearm originate via a common tendon from the medial epicondyle, while the common extensor/supinator tendon originates on the lateral epicondyle. The supinator muscle arises from the lateral epicondyle, the radial collateral and annular ligaments and the proximal-lateral aspect of the ulna. It then encircles the proximal radius and inserts along its proximal aspect.
Tendons and Muscles: MR Imaging Technique
Axial images are excellent for evaluating the biceps and brachialis tendons while the common flexor and extensor tendons are well evaluated in both the axial and the coronal planes. The triceps tendon is best assessed on sagittal images. Tendons should be of low signal intensity on all MR imaging sequences but, like ligaments, may demonstrate magic angle artifacts on „short TE” images (T1, proton density, gradient echo). Acute muscle pathology will be most conspicuous on fat-saturated T2-weighted images. Chronic muscle atrophy is best identified on T1-weighted non-fatsaturated images.
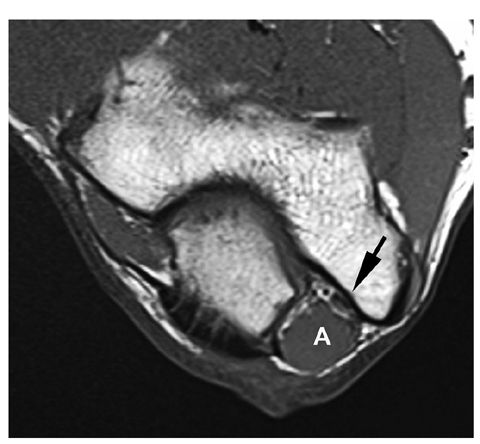
Tendons and Muscles: Potential Pitfalls
The anconeus epitrochlearis is an anomalous muscle, seen in approximately 10% of individuals, that lies along the medial aspect of the olecranon. While this is usually an asymptomatic normal variant, it may produce symptoms of ulnar neuropathy due to compression of the nerve within the adjacent cubital tunnel (Fig. 12) [51].