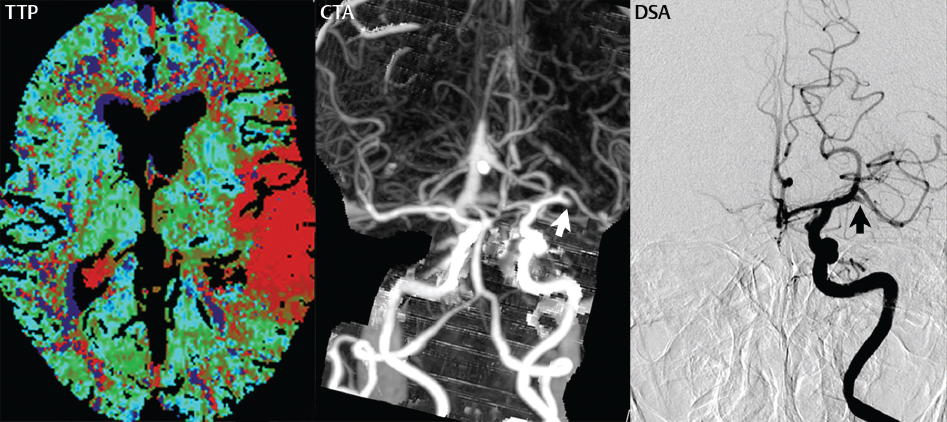
In young patients, the etiologies for cerebral infarction are many and varied, in distinction to adults. Leading causes include congenital and acquired heart disease, together with sickle cell disease. In the elderly, infarcts are most often due to atherosclerosis, with vessel occlusion due to either thrombosis or embolism (Fig. 1.55).
Fig. 1.55 Hyperacute distal MCA territory infarct, evaluation by CT. This 79-year-old woman presented 1.5 hours prior to the initial imaging evaluation with clinical signs of ischemia in the left MCA territory. The unenhanced CT (not shown) was grossly unremarkable. The time to peak (TTP) image reveals delayed perfusion in nearly the entire left MCA territory, with the exception of the lenticulostriate artery distribution. CBV was normal (not shown). CTA reveals thromboembolic occlusion (white arrow) of the distal left M1 segment of the MCA. The occlusion (black arrow) was confirmed on DSA. Following mechanical thrombectomy (3 hours following the CT), flow to the left MCA and its branches was fully restored (image not shown).
Common areas of atherosclerotic involvement include the carotid bifurcation, distal internal carotid artery, and middle cerebral artery. Risk factors for infarction in an adult include high blood pressure, high cholesterol, smoking, diabetes, obesity, cardiovascular disease, oral contraceptives, and cocaine. The clinical presentation is that of an acute neurologic deficit.
Infarction involving the precentral gyrus (primary motor cortex) leads to contralateral motor deficits. Infarction in the left inferior frontal gyrus (specifically in Broca′s area, the part of the brain responsible for speech production) causes an expressive aphasia. Infarction in the left posterior superior temporal gyrus (specifically in Wernicke′s area) causes receptive aphasia. The latter two statements apply to patients who are left-hemisphere dominant.
Arterial Territory Infarcts
Infarcts in the major arterial territories are easily recognized due to their arterial distribution and their involvement of both gray and white matter. MCA infarcts are most common, followed by PCA infarcts. Of the three major arterial territories, ACA infarcts are by far the least common. The MCA supplies the lateral cerebral hemispheres, with the lenticulostriate arteries (arising from the M1 segment) supplying the globus pallidus and putamen and the anterior limb of the internal capsule. The PCA can originate from the tip of the basilar artery (80%) or in the case of a fetal origin (20%) directly from the internal carotid artery. The PCA supplies the posteroinferior temporal lobe, medial parietal lobe, occipital lobe, and portions of the brainstem, thalamus, and internal capsule (Fig. 1.56). The ACA supplies the anterior putamen, caudate nucleus, hypothalamus, corpus callosum, and medial surface of the cerebral hemisphere (Fig. 1.57).
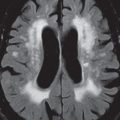
Fig. 1.56 Posterior cerebral artery (PCA) infarction, early subacute. There is both vasogenic edema and cytotoxic edema, as demonstrated by respectively high signal intensity on the T2- and the diffusion-weighted scans, in the entirety of the left PCA distribution. In this instance, infarcts of the same time frame are also seen in the left thalamus (white arrow), which is supplied by the posterior thalamoperforators (which originate from the P1 segment of the PCA). There is also hemorrhage (black arrow) within the lesion, seen with low signal intensity due to a T2* effect.Fig. 1.57 Anterior cerebral artery (ACA) infarct, early subacute. On FLAIR, there is abnormal high signal intensity in the medial frontal lobe (ACA territory) on the right, involving both gray and white matter, with mild mass effect upon the frontal horn of the lateral ventricle. There is corresponding abnormal hyperintensity on DWI, reflecting cytotoxic edema (confirmed to be restricted diffusion on the ADC map). This anatomic distribution lies within, and forms part of, the ACA territory. Also present is loss of brain substance and mild gliosis in the left parietal region, consistent with a chronic watershed infarct.
The posterior inferior cerebellar artery (PICA) arises from distal vertebral artery and supplies the retro-olivary (lateral) medulla, inferior vermis, tonsil, and posterior inferior portion of the cerebellar hemisphere (Fig. 1.58). The most frequent cause of a PICA infarct is thrombosis of the vertebral artery. The anterior inferior cerebellar artery (AICA) supplies a small portion of the cerebellum, anteriorly and inferiorly. Its territory is often referred to as being in equilibrium with PICA, specifically the larger the PICA territory, the smaller the AICA territory (and vice versa). The remaining arterial territory in the cerebellum is that of the superior cerebellar artery (SCA), which supplies the superior half of the cerebellum (and parts of the midbrain) (Fig. 1.59) and arises from the basilar artery just proximal to the posterior cerebral artery. The largest two cerebellar, arterial territories are that of the SCA and PICA. Concerning territorial infarcts in the cerebellum, PICA is most common, followed by the SCA, with infarcts of AICA being uncommon. In the elderly, chronic small cerebellar infarcts are commonly detected on MR, and are seen in both major territories.
Fig. 1.58 Posterior inferior cerebellar artery (PICA) infarction. On a sagittal T1-weighted scan (part 1), abnormal low signal intensity (arrow) is seen involving the inferior half of the cerebellum, consistent with a subacute PICA territory infarct. This is the most common territorial infarct seen in the cerebellum. In a different patient (part 2), a chronic left PICA infarct is noted. There is absence of brain substance (cystic encephalomalacia) in the region of the posteroinferior cerebellum on the left. Note that the involved cerebellum includes the cerebellar tonsil and a portion of the vermis. There is mild loss of substance involving the left medulla, with a tiny area of cystic encephalomalacia, with the lower medulla supplied by PICA in about half of cases. Note the spared anterior cerebellum at this level, in the AICA territory.Fig. 1.59 Superior cerebellar artery infarct. This late subacute infarct demonstrates low density on CT and high signal intensity on the T2-weighted scan, indicative of vasogenic edema. The area of infarction is also high signal intensity on DWI (confirmed as restricted diffusion on the ADC map, not shown), consistent with accompanying cytotoxic edema. Note that the level illustrated is within the superior half of the cerebellum, the superior cerebellar artery distribution, and that nearly the entirety of the right side is involved, with a small infarct as well on the left. Mild mass effect upon the pons, and the extent of ischemia on the left, are better depicted on MR.
Lacunar Infarcts
Lacunar infarcts are small, deep cerebral infarcts, most frequently seen with hypertension. They result from occlusion of small penetrating arteries arising from the major cerebral arteries, and most commonly involve the basal ganglia (Fig. 1.60), internal capsule, thalamus (Fig. 1.61), and brainstem (Fig. 1.62). The blood supply to the pons is mainly from the basilar artery via small paramedian and circumferential penetrating branches. Infarcts in the pons are most frequently unilateral, paramedian, and sharply marginated at the midline. Bilateral pontine infarcts, which are less common, remain paramedian in distribution. Lateral pontine infarcts are uncommon. The differential diagnosis for a unilateral pontine lesion includes multiple sclerosis (MS), whereas for bilateral central lesions the differential diagnosis includes central pontine myelinolysis and pontine glioma.
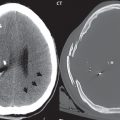
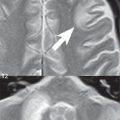
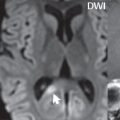
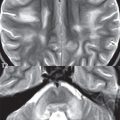
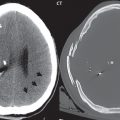
Fig. 1.60 Chronic lacunar infarct. A focal very low attenuation lesion is seen within the caudate head on CT, with corresponding high signal intensity on the T2-weighted scan, consistent with a chronic cavitated infarct. A caveat however is that very low attenuation on rare occasion corresponds to edema in an early subacute infarct, with CT both less sensitive for detection of ischemia and also much less specific in regard to dating when compared to MR.Fig. 1.61 Acute thalamic infarction. There is restricted diffusion, with abnormal high signal intensity on the diffusion-weighted image, in this small acute, right sided, lacunar infarct (black arrow). Unenhanced CT, obtained with a 4-mm slice thickness, does not visualize the lesion, which is common due to the lower sensitivity of this modality (and its insensitivity to cytotoxic edema). Note that on thinner section images (2 mm), obtained during bolus contrast administration (CTA), that the infarct (white arrow) can be recognized in retrospect due to slight lower attenuation in comparison with adjacent normal brain.Fig. 1.62 The anatomic spectrum of lacunar infarction. In the first patient, on DWI, high signal intensity is seen both in the lentiform nucleus (globus pallidus and putamen) and the caudate head, a common imaging appearance. The caudate head lesion is also shown on FLAIR to be high signal intensity, dating this lesion as acute to subacute in time frame. The caudate infarct, however, cannot be differentiated on the basis of signal intensity on the FLAIR scan from the marked accompanying periventricular white matter gliosis. In the second and third patients, respectively, thalamic (white arrow) and pontine lacunar infarcts are seen with high signal intensity on DWI. Note the sharp demarcation, vertically along the median raphe, of the pontine infarct, a common imaging appearance. In the fourth patient, a lateral medullary infarct (white arrow) is seen with hyperintensity on both DWI and T2-weighted scans.
Only gold members can continue reading. Log In or Register to continue