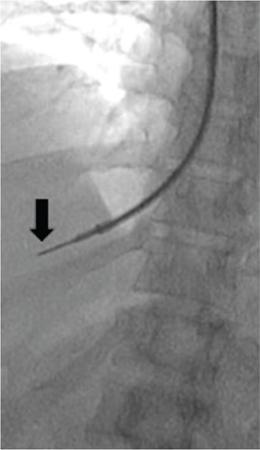
Amar Mukund, Shaleen Rana Portal hypertension (PH) is an inevitable complication of chronic liver disease. Chronic liver disease results in increased vascular resistance due to fibrosis and increased sinusoidal tone. Associated increase in portal flow is seen due to hyperdynamic circulation and expanded plasma volume which is a result of splanchnic vasodilatation and neoangiogenesis. Splanchnic vasodilatation further activates the vasoactive pathways secondary to systemic underfilling, resulting in ascites and renal derangement. As the portal pressure increases there is a transition from the subclinical to the clinical phase. Increasing portal pressure causes a gradient between the portal vein and inferior vena cava (IVC) known as the portal pressure gradient (PPG). The increasing gradient coupled with neoangiogenesis opens up portosystemic collaterals and formation of varices. The asymptomatic stage is called compensated cirrhosis (CC) or compensated advanced chronic liver disease. The patients with hepatic venous pressure gradient (HVPG) between 5 and 10 mm Hg are labelled as mild PH while those with HVPG >10 mm Hg are labelled as clinically significant portal hypertension (CSPH). The onset of CSPH is associated with various complications of PH. The causes of PH have been classified into (1) Prehepatic (portal, splenic or mesenteric vein thrombosis), (2) Intrahepatic (diseases like viral/alcoholic hepatitis) and (3) Posthepatic (Budd–Chiari syndrome). Complications of PH like ascites, encephalopathy and variceal bleeding increase the morbidity and mortality in patients with chronic liver disease and are directly proportional to the increasing portal pressure. Early recognition and diagnosis of PH and its types can help to prevent development of complications in an asymptomatic patient and to treat the complications in a symptomatic patient. Subclinical PH usually has no positive signs on examination. Presence of splenomegaly, abdominal wall collaterals, ascites and spider naevi suggest advanced disease. Various parameters like albumin, international normalized ratio (INR), platelets and liver function tests have been used in various combinations (Fibroindex, AST – platelet ratio index and Fibrosis – 4) and attempts have been made to correlate with progression of fibrosis and PH with reasonable degree of success. Ultrasound and contrast-enhanced CT/MRI are good in depicting the complications of chronic liver disease however none of the modalities measures the HVPG and do not correlate well with HVPG. TE can be used as a tool for assessing liver stiffness in patients with chronic liver disease. Baveno VI consensus workshop recommends that TE values >15 kPa suggests CC and screening endoscopy can be avoided in patients with liver stiffness <20 kPa and platelet count >1,50,000 as these patients have very lower risk of varices. The above-mentioned noninvasive modalities lack the sensitivity and specificity of HVPG and none of these modalities directly measure the HVPG. HVPG is an invasive technique which helps in determining portal pressure using a catheter placed in one of the hepatic veins. When a catheter is wedged in the hepatic vein the proximal column of blood reflects the pressure within the hepatic sinusoids. In cirrhosis, there is loss of normal connections within the sinusoids and the wedged hepatic venous pressure (WHVP) represents the portal pressure. Hepatic vein pressure gradient (HVPG) is calculated by subtracting free hepatic venous pressure (FHVP) from the WHVP. HVPG measurement is currently considered the gold standard for measurement of portal venous pressure in chronic liver disease. HVPG is helpful in diagnosing and measuring the severity of PH. HVPG predicts the severity of cirrhosis, clinical course in chronic hepatitis B and C infections and the development of complications. It is a surrogate clinical marker and has been used for prognostication and treatment response. HVPG >10 mm Hg is associated with formation of oesophagal varices while HVPG >12 mm Hg is associated with increased risk of variceal bleeding and ascites. A baseline HVPG of ≥16 is associated with increased risk of death irrespective of presence or absence of varices with no bleeding. Patients with HVPG ≥20 mm Hg presenting with variceal bleeding are more likely to have early rebleeding or inability to control bleeding than patients with HVPG <20 mm Hg. There is a higher transfusion requirement, longer intensive care unit stay and increased mortality in patients with HVPG ≥20 mm Hg. Decrease in HVPG to ≤12 mm Hg with pharmacotherapy or improving liver functions prevents variceal bleeding and reduces the size of existing varices. Similarly, ≥20% reduction in baseline HVPG reduces the risk of bleeding, variceal rebleed, ascites and mortality. Serial measurements of HVPG have been used for assessment of response to Hepatitis C treatment and effect of pharmacological therapy in lowering portal pressure. Several studies showed that there was significant reduction in HVPG posttreatment for hepatitis C infections. Preoperative use of HVPG in patients undergoing hepatectomy has been found to predict post hepatectomy decompensation and is more likely to occur in patients with CSPH (HVPG >10 mm Hg). HVPG also predicts recurrence or onset of hepatitis C cirrhosis in transplant patients and HVPG >6 mm Hg in these patients is associated with disease progression. HVPG measurement via hepatic vein catheterization is simple, safe and reproducible technique with immense clinical benefit. Hepatic vein catheterization is done under conscious sedation in a daycare setting with continuous monitoring of the vitals during the procedure. The patient should be fasting for minimum 6 hours. Venous access (Internal jugular, femoral or ante cubital vein) is secured under local anaesthesia. A balloon-tipped catheter is advanced into the right hepatic vein through the internal jugular vein (IJV) or IVC over a guidewire. Contrast is injected through the balloon catheter to confirm the position of the catheter and the diameter of the vein. FHVP is measured by letting the catheter tip float freely in the hepatic vein for at least 15 seconds within 5 cm of the hepatic vein ostium. WHPV is measured by inflating the balloon so that it is well opposed to the venous walls and the pressure tracing is stable for a minute (Fig. 9.26.1). After measuring the pressure adequate occlusion of the vein is confirmed by injecting 3–5 mL contrast slowly which should result in a wedge sinusoidogram, no reflux via collateral veins, absence of venous waveform and no blood on applying suction through the catheter. In the event of inadequate occlusion, the pressure is measured again and occlusion is verified again. Three readings are taken if the variation is ≤1 mm Hg and a mean of the values is considered. Permanent recording of the tracing using a multichannel recorder is done. The HVPG is calculated by subtracting FHVP from the WHVP. The advantage of measuring the gradient is that it is unaffected by changes in abdominal pressure, ascites or the hydration status of the patient. Venous pressure should also be measured in the IVC and the right atrium (RA). The IVC pressure should be measured at the level of the hepatic vein ostia because the pressure may be higher inferiorly due to compression of the IVC by hepatic parenchymal hypertrophy. The gradient between the hepatic veins and the RA should not be more than 2 mm Hg. If the gradient is >2 mm Hg then one must suspect a narrowing or a web in the hepatic vein or the IVC. Using RA pressures for HVPG measurement has the advantages of easy reproducibility and that it measures the actual portosystemic gradient. WHVP should be separately mentioned as it represents the pressure of blood in the varices and hence risk of variceal rupture. Patients coughing, movement or talking should also be recorded as it may cause artefacts while recording a trace. After successfully measuring the pressures the catheter and the sheath is removed and manual compression of the puncture site is done till the oozing stops followed by immobilization of the part for at least 4 hours. Some points to be kept in mind while measuring HVPG. HVPG measurement is a safe procedure with no major complication or mortality. Puncture site leakage and hematoma of the access vessel are the common complications. Rare complications are vasovagal syncope and arteriovenous fistula formation. Most of the complications can be avoided by using ultrasound for puncture of the access vessels and adequate postprocedural compression. Self-limiting supraventricular arrhythmias may be seen when the wire or the catheter traverses the RA. TJLB was introduced to reduce the complications associated with percutaneous liver biopsy (PLB) in patients with ascites, coagulopathy or in patients whose percutaneous biopsy had failed. Transjugular biopsy is now an acceptable and established technique for obtaining biopsy from the liver with no incidence of major complications. TJLB is done as a daycare procedure. Patient has to be fasting for 6 hours and an informed consent should be taken. The patient is shifted to a procedure room/cath-lab and the right neck is cleaned and draped. Continuous monitoring of the vitals is done throughout the procedure. Under local anaesthesia right IJV is accessed and a 10 F vascular sheath is introduced. Through the sheath, right hepatic vein is accessed using a 5F catheter and J tip floppy guidewire (Terumo, Japan). A contrast run is taken to confirm the position of the catheter in the right hepatic vein. The floppy guidewire is exchanged with a 0.035-inch stiff guidewire over which a curved stiff TJLB cannula is advanced. The stiff TJLB cannula is wedged against the wall of the hepatic vein. Wedging prevents the needle from slipping while taking a tissue core. This is followed by introduction of the semiautomatic coaxial biopsy gun (Fig. 9.26.2). Two to three cores are taken. The needle should be directed anteriorly when taking a biopsy from the right hepatic vein and laterally while taking biopsy from the middle hepatic vein. A contrast run is taken postprocedure. Postprocedure the neck access site is compressed manually and patient is monitored for 4–6 hours. If patient complains of severe pain not relieved by analgesics or if there is any tachycardia/fall in blood pressure, ultrasound should be done to rule out hemoperitoneum. Following important steps not to be overlooked.
9.26: Interventions in portal hypertension
Portal hypertension
Assessment of portal hypertension
Clinical examination
Laboratory investigations
Imaging
Transient elastography (TE)
HVPG
Indications
Contraindications
Technique

Complications
Transjugular liver biopsy
Introduction
Indications
Relative contraindications
Technique
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


