Intramural Benign Esophageal Tumors
Michael P. Federle, MD, FACR
Key Facts
Imaging
Types include leiomyoma, GI stromal tumor, granular cell, lipoma, hemangioma, hamartoma
Fluoroscopic-guided barium studies
Discrete mass; solitary (most common) or multiple
Round or ovoid filling defects sharply outlined by barium on each side (en face view)
Narrowed (tangential view) or stretched and widened (en face view) esophageal lumen
Smooth surface lesion, with upper and lower borders of lesion forming right or slightly obtuse angles with adjacent esophageal wall (profile view)
Overlying mucosa may ulcerate
Leiomyoma: ± amorphous or punctate calcifications
Esophageal GIST
May be large mass
May ulcerate with gas ± contrast medium entering cavity
CT: Discrete mass in wall; no signs of invasion or metastases
Helps distinguish lipoma (fat density) and other mediastinal masses (e.g., mediastinal cyst)
Top Differential Diagnoses
Mediastinal tumor
Normal mediastinal structures
Esophageal carcinoma
Foreign body
Clinical Issues
Asymptomatic: No treatment
Large symptomatic lesions: Enucleation or esophageal resection with gastric interposition
Diagnostic Checklist
Most intramural masses are benign (unlike gastric tumors)
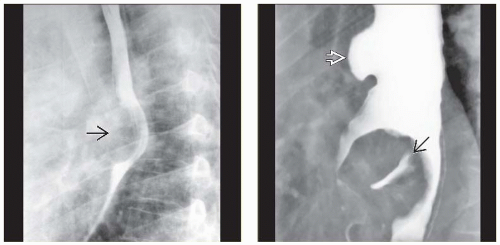 (Left) Film from a barium esophagram demonstrate a mass  causing eccentric narrowing of the distal lumen. The mass forms obtuse angles with the wall, and the esophageal folds and mucosa are intact. A leiomyoma was enucleated endoscopically. (Right) Single contrast esophagram shows an en face view of an intramural mass in the distal esophagus with central ulceration causing eccentric narrowing of the distal lumen. The mass forms obtuse angles with the wall, and the esophageal folds and mucosa are intact. A leiomyoma was enucleated endoscopically. (Right) Single contrast esophagram shows an en face view of an intramural mass in the distal esophagus with central ulceration  due to leiomyoma. The traction diverticulum due to leiomyoma. The traction diverticulum  is an incidental finding. is an incidental finding. |
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


