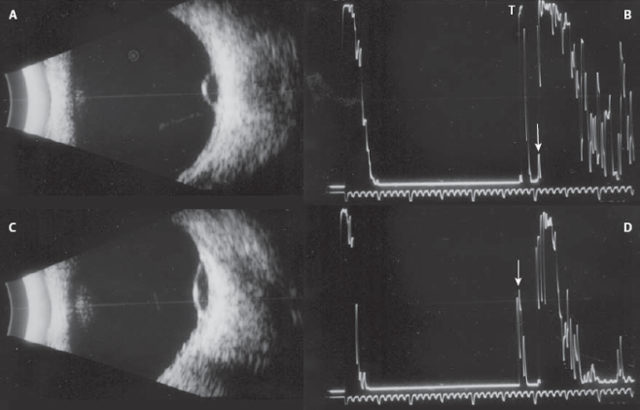
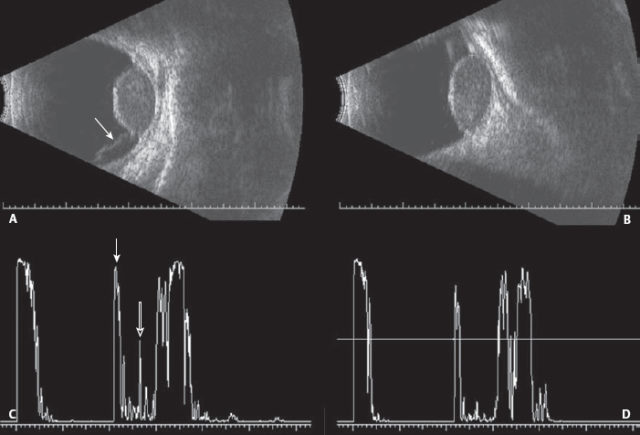
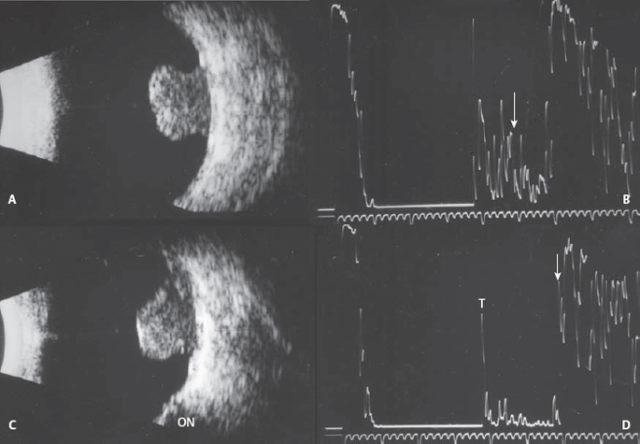
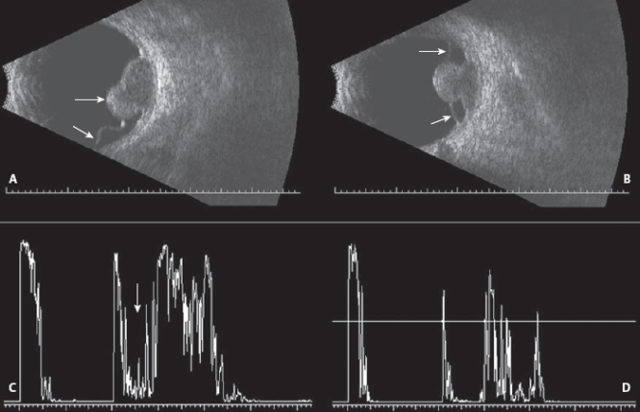
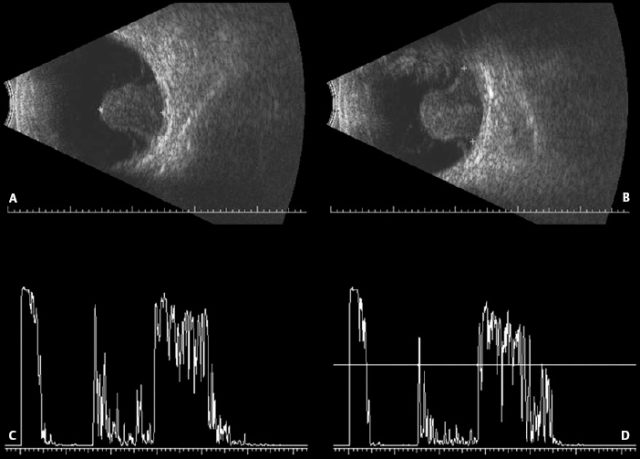
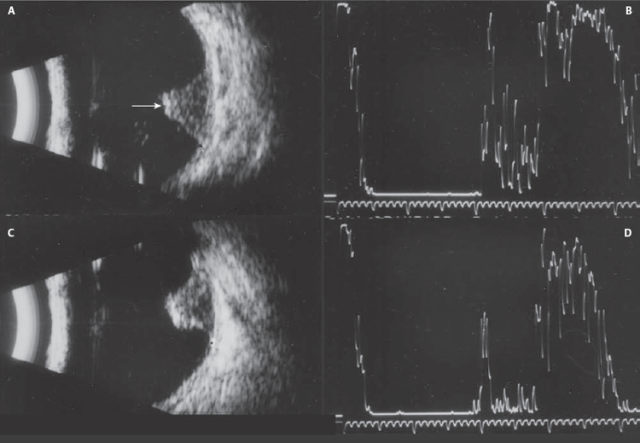
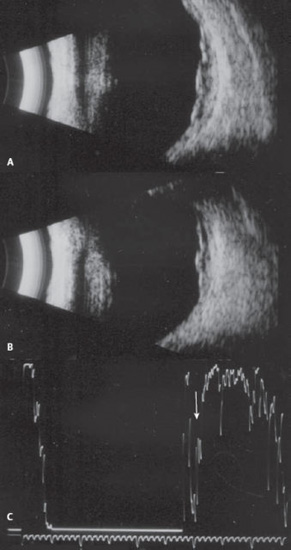
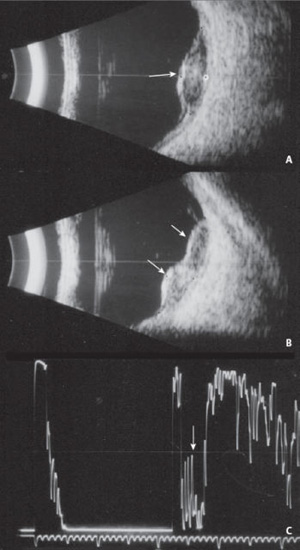
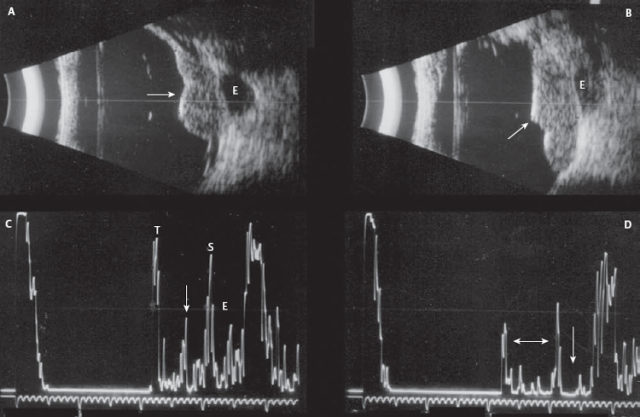
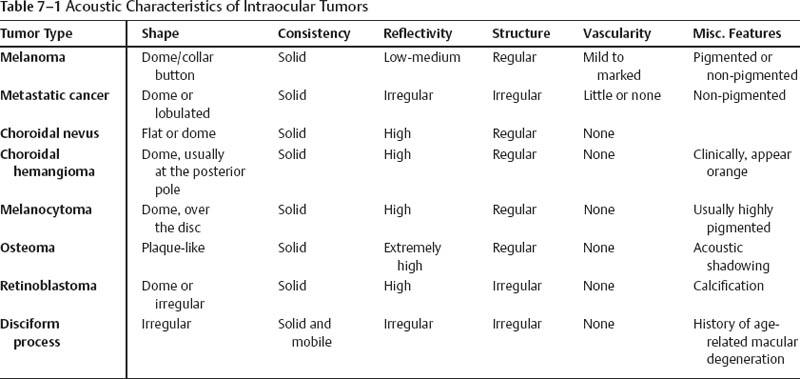
7 Many intraocular tumors are easily distinguishable from one another ophthalmoscopically when the media is clear. Some mimic one another and are more difficult to diagnose, and if the media is not clear, ophthalmoscopic differentiation may be impossible. Standardized echography can play an important role in confirming the diagnosis, obtaining accurate measurements of newly discovered lesions, and monitoring changes that may occur over time. Information concerning the patient’s history, as well as the clinical findings such as location, pigmentation, and presence of vitreous hemorrhage and/or retinal detachment are all useful pieces of information for the echographer. For instance, if hemorrhage is present in the vitreous or beneath the retina, the likelihood of a lesion being a metastatic carcinoma is diminished. Echographically, intraocular tumors display different acoustic characteristics because of their vastly different histopathologic compositions. These distinguishing features are most appreciated with the standardized A-scan at the tissue sensitivity setting. The B-scan is most useful in determining the topographic features of tumors, such as shape, location and extension. The basal diameter is determined using both transverse (lateral dimension) and longitudinal (radial dimension) scans. Sometimes gross estimation of the height can also be performed using contact B-scan, but the standardized A-scan provides the most accurate measurements from the surface of the tumor to the inner sclera. The structure (distribution of cells), the reflectivity (size of the cells), and the presence or absence of vascularity can be appreciated best with the standardized A-scan. The typical echographic features of intraocular tumors and pseudotumors are described in Table 7–1. Keep in mind that sometimes a lesion’s characteristics do not conform to what is considered typical. In these cases, it is important for the echographer to note any atypical features and correlate these findings to the clinical history and appearance. On the following pages are selected cases of intraocular tumors with descriptions of the echographic findings. Byrne SF, Green RL. Second Edition: Ultrasound of the Eye and Orbit. St. Louis: Mosby Yearbook; 2002 Farah ME, Byrne SF, Hughes JR. Standardized echography in uveal melanomas with scleral or extraocular extension. Arch Ophthalmol 1984;102:1482–1485 Harbour JW, Murray TG, Byrne SF, et al. Intraoperative echographic localization of iodine 125 episcleral radioactive plaques for posterior uveal melanoma. Retina 1996;16:129–134 Schachat AP, DiBernardo C. Management of a patient with a small choroidal melanoma. Wilmer Retina Update 1995;1:13–16 Figure 7–1 Dome-shaped. Three examples of different-sized dome-shaped lesions. (A) Small dome-shaped lesion in transverse scan showing the lateral extent. (B) High spike from the surface of the tumor (T) and very low internal reflectivity (arrow). (C) Longitudinal scan showing the radial extent. (D) The gain has been reduced to obtain an accurate measurement from the surface of the tumor (arrow). Figure 7–2 Dome-shaped. (A) Transverse scan of dome-shaped tumor with shallow retinal detachment at the inferior edge of the lesion (arrow). (B) Longitudinal scan showing the radial extent of the lesion. (C) A-scan showing the high spike from the surface of the lesion (closed arrow) and the low reflectivity consistent with melanoma (open arrow). (D) The gain has been reduced to obtain an accurate measurement. Figure 7–3 Collar button. (A) Transverse B-scan showing the mushroom shape of the tumor. (B) Tissue sensitivity. Note the low internal reflectivity (arrow). (C) Longitudinal B-scan showing the location along the meridian in relation to the optic nerve (ON). (D) Measuring sensitivity; arrow, innerscleral spike; T, tumor surface. Figure 7–4 Collar button. If a melanoma breaks through Bruch’s membrane, a “collar button” configuration results. These collar buttons can vary in size, also in configuration, depending on the area where the rupture occurred. (A) Transverse showing the collar button at the more inferior edge of the tumor (top arrow) and the adjacent retinal detachment (bottom arrow). (B) Longitudinal scan showing the lesion and the retinal detachment anterior and posterior to the lesion (arrows). (C) Standardized A-scan at tissue sensitivity showing the low reflectivity (arrow). (D) Measuring sensitivity A-scan. Figure 7–5 Collar button. (A) Transverse scan. (B) Longitudinal scan. (C) A-scan at tissue sensitivity to evaluate the height of the internal spikes. (D) A-scan at measuring sensitivity. Figure 7–6 Collar button. This patient was a monocular, mentally handicapped man whose caregivers noticed a decrease in his ambulatory level. Clinically, he had a dense cataract. (A) Echographically, there was a massive collar button–shaped tumor. (B) The internal structure was typical for melanoma. Figure 7–7 Peaked. This patient presented with vitreous hemorrhage. On clinical examination, there was suggestion of retinal detachment. (A) Transverse B-scan at decreased gain, showing a peaked tumor (arrow). (B) A-scan showing low internal reflectivity. (C) Longitudinal B-scan. (D) Decreased gain for the measurement. Figure 7–8 Diffuse melanoma. (A) Transverse image showing the large lateral extent of this diffuse melanoma. (B) Longitudinal scan. (C) Although the lesion is not very elevated, which is usually the case in diffuse lesions, the reflectivity is low (arrow). Figure 7–9 Lobulated. (A) In transverse (cross-section) view the tumor appears to be dome-shaped (arrow). (B) The longitudinal scan showing that it is actually bi-lobed (arrows). (C) A-scan showing low reflectivity (arrow). Figure 7–10 Extrascleral extension. (A)
Intraocular Tumors
 Suggested Readings
Suggested Readings

![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


