Intravascular contrast media
Historical development of radiographic agents
The first report of opacification of the urinary tract after intravenous (i.v.) injection of a contrast agent appeared in 1923 using an i.v. injection of 10% sodium iodide solution, which was at that time prescribed for treatment of syphilis and was excreted in the urine. In 1928 German researchers synthesized a compound with a number of pyridine rings containing iodine in an effort to detoxify the iodine. This mono-iodinated compound was developed further into di-iodinated compounds and subsequently in 1952 the first tri-iodinated compound, sodium acetrizoate (Urokon), was introduced into clinical radiology. Sodium acetrizoate was based on a 6-carbon ring structure, tri-iodo benzoic acid, and was the precursor of all modern water-soluble contrast media.
Until the early 1970s all contrast media were ionic compounds and were hypertonic with osmolalities of 1200–2000 mosmol kg−1 water, 4–7 × the osmolarity of blood. These are referred to as high osmolar contrast media (HOCM) and distinguished by differences at position 5 of the anion and by the cations sodium and/or meglumine. In 1969 Almén first postulated that many of the adverse effects of contrast media were the result of high osmolality and that by eliminating the cation, which does not contribute to diagnostic information but is responsible for up to 50% of the osmotic effect, it would be possible to reduce the toxicity of contrast media.
Conventional ionic contrast media had a ratio of three iodine atoms per molecule to two particles in solution, i.e. a ratio of 3 : 2 or 1.5 (Table 2.1). In order to decrease the osmolality without changing the iodine concentration, the ratio between the number of iodine atoms and the number of dissolved particles must be increased.
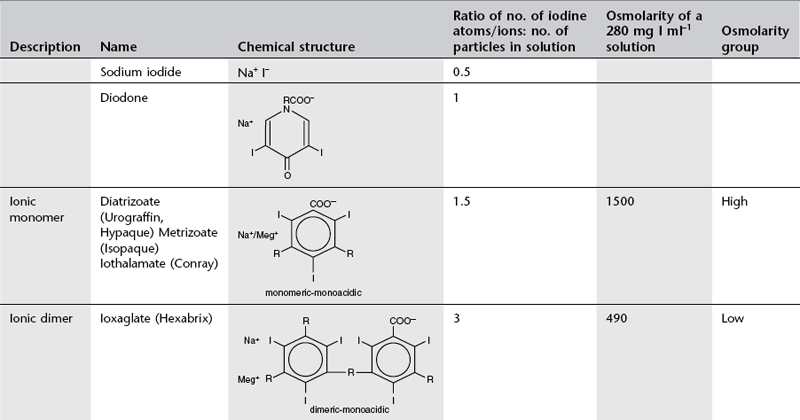
Development to produce low osmolar contrast medium (LOCM) proceeded along two separate paths (Table 2.1). The first was to combine two tri-iodinated benzene rings to produce an ionic dimer with six iodine atoms per anion; ioxaglate (Hexabrix). The alternative, more successful, approach was to produce compounds that do not ionize in solution and so do not provide radiologically useless cations. Low osmolar contrast media of this type are referred to as non-ionic. These include the non-ionic monomers iopamidol (Niopam, Iopamiron, Isovue and Solutrast), iohexol (Omnipaque), iopromide (Ultravist), iomeprol (Iomeron) and ioversol (Optiray), which are now used widely.
For both types of LOCM the ratio of iodine atoms in the molecule to the number of particles in solution is 3 : 1 and osmolality is theoretically halved in comparison with high osmolar contrast material (HOCM). However, because of aggregation of molecules in solution the measured reduction is only approximately one-third (Fig. 2.1).
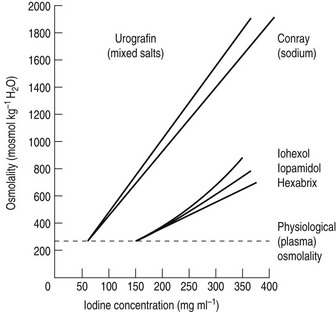
Figure 2.1 A plot of osmolality against iodine concentration for new and conventional contrast media. From Dawson et al.1 (Reproduced by courtesy of the editor of Clinical Radiology.)
Further research led to the introduction of non-ionic dimers – iotrolan (Isovist) and iodixanol (Visipaque). These have a ratio of six iodine atoms for each molecule in solution with satisfactory iodine concentrations at iso-osmolality; they are, therefore, called iso-osmolar contrast media. The safety profile of the iso-osmolar contrast agents is at least equivalent to LOCM, but any significant advantage of iso-osmolar contrast remains controversial.2
The low- and iso-osmolar contrast media are 5–10 times safer than the HOCM3 and are used routinely in clinical practice. With development having reached the stage of iso-osmolality, further research is now targeted on decreasing the chemotoxicity and viscosity of iodinated contrast media.
References
1. Dawson, P, Grainger, RG, Pitfield, J. The new low-osmolar contrast media: a simple guide. Clin Radiol. 1983; 34:221–226.
2. Morcos, SK. Contrast-induced nephropathy: are there differences between low osmolar and iso-osmolar iodinated contrast media? Clin Radiol. 2009; 64:468–472.
3. The Royal College of Radiologists. Standards for Intravenous Iodinated Contrast Administration to Adult Patients, 2nd ed. BFCR(10)4. London: The Royal College of Radiologists; 2010.
Adverse effects of intravenous water-soluble contrast media
The toxicity of contrast media is a function of osmolarity, ionic charge (ionic contrast agents only), chemical structure (chemotoxicity) and lipophilicity.
Adverse reactions after administration of non-ionic iodinated contrast media are rare, occuring in less than 1% of all patients.1 Of these reactions, the vast majority are mild and self-limiting. The incidence of moderate or severe non-ionic contrast reactions is less than 0.001%.2
Toxic effects on specific organs
Soft-tissue toxicity
Pain, swelling, erythema and even sloughing of skin may occur from extravasated contrast medium. The risk is increased when pumps are used to inject large volumes of contrast medium during computed tomography (CT) examinations. Treatment should consist of the application of cold packs and elevation of the limb. Systemic steroids, non-steroidal anti-inflammatory drugs and antibiotics have all been shown to be useful.
Cardiovascular toxicity
1. Intracoronary injection of contrast media may cause significant disturbance of cardiac rhythm.
2. Increased vagal activity may result in depression of the sino-atrial and atrio-ventricular nodes, causing bradycardia or asystole.
3. Injection of hypertonic contrast medium causes significant fluid and ion shifts. Immediately after injection there is a significant increase in serum osmolality. This causes an influx of water from the interstitial space into the vascular compartment, an increase in blood volume, an increase in cardiac output and a brief increase of systemic blood pressure. Peripheral dilatation may cause a more prolonged fall of blood pressure. Injection into the right heart or pulmonary artery causes transitory pulmonary hypertension and systemic hypotension; injection into the left ventricle or aorta causes brief systemic hypertension followed by a more prolonged fall.
Haematological changes
1. In the presence of a high concentration of contrast medium, such as withdrawal of blood into a syringe of contrast medium, damage to red cell walls occurs and haemolysis follows. Haemolysis and haemoglobinuria have been reported following angiocardiography. It is advisable not to re-inject blood that has been mixed with contrast medium.
2. Red cell aggregation and coagulation may occur in the presence of a high concentration of contrast medium, e.g. 350 mg I ml−1. However, disaggregation occurs easily and this is not likely to be of any clinical significance.
3. Contrast media may impair blood clotting and platelet aggregation. Low- and iso-osmolar contrast media have a minimal effect compared to HOCM.3
4. Contrast media have a potentiating effect on the action of heparin.
5. Thrombus formation occurs when blood is mixed with LOCM during injection. However, the role of the syringe is also significant; thrombus formation is maximal when blood is slowly withdrawn into a syringe so that it layers on top of the contrast medium, against the wall of the syringe, therefore this should be avoided. Activation of coagulation by the tube material probably plays a significant role.
6. Contrast media have been shown to cause HbSS blood to sickle in vitro. Iso-osmolar contrast agents have a lesser effect and their use is indicated in this disease.4 Beneficial diagnostic imaging with intravascular contrast can be performed without significant increased risk of serious complication in patients with sickle cell disease.5
7. When red blood cells are placed in a hypertonic contrast medium, water leaves the interior of the cells by osmosis and they become more rigid and less deformable. Iso-osmolar solutions also have an effect on red cell deformability, indicating that there may also be a chemical effect. Red cells that deform less easily are less able to pass through capillaries and may occlude them. This is the explanation for the transient rise in pulmonary arterial pressure during pulmonary arteriography and may also be a factor in contrast-induced nephropathy.
8. Transient eosinophilia may occur 24–72 h after administration of contrast medium.
Nephrotoxicity
Contrast-induced nephropathy (CIN) is one of the most serious adverse effects associated with the use of intravascular contrast media and is defined as an impairment of renal function (increase in serum creatinine >25% baseline value or 44 µmol l−1)6 occurring within 3 days of contrast administration in the absence of an alternative aetiology. In those affected, the serum creatinine concentration starts to rise within the first 24 h, reaches a peak by 2–3 days and usually returns to baseline by 3–7 days. In rare cases patients may need temporary or permanent dialysis. The mechanisms of CIN are summarized below:7
1. Altered vascular haemodynamics:
(a) adverse cardiotoxic effects
(b) increased peripheral vasodilatation
(c) renal vascular bed changes (increased blood flow followed by a more prolonged decrease)
(d) increased rigidity of red cells.
2. Glomerular and tubular injury:
3. Interference with intratubular fluid volume and viscosity.
It was hoped that the iso-osmolar contrast agents might be less nephrotoxic than LOCM, however clinical trials have so far yielded conflicting results.8 CIN has a complex aetiology and the positive benefit of reduction in osmolarity achieved with iso-osmolar contrast medium may be negated by the accompanying increase in viscosity.
There are a number of predisposing factors in CIN:
1. The single most important risk factor is pre-existing impairment of renal function; patients with normal renal function are at very low risk. A guide level of eGFR < 60 ml/min/1 is recommended to indicate renal impairment3,9 (Fig. 2.2)
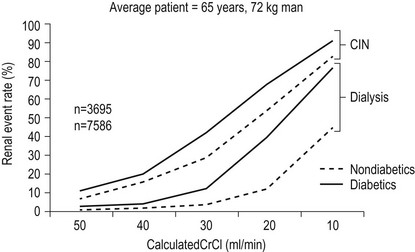
Figure 2.2 Validated risk of CIN and dialysis after diagnostic angiography and ad hoc angioplasty by creatinine clearance (CrCl) and diabetes. This assumes a mean contracts dose of 250 ml and a mean age of 65. (Adapted from Reference 9, with permission from Elsevier.)
2. Diabetes mellitus
3. Dehydration
4. Sepsis
5. Age > 70 years
6. Use of very large doses of contrast medium
7. Multiple myeloma
8. Concomitant use of nephrotoxic drugs
9. Vascular disease.
A further hazard for patients who suffer impairment of renal function as a result of intravascular iodinated contrast is reduced renal clearance of other drugs, e.g. metformin, an oral hypoglycaemic drug which is exclusively excreted via the kidneys. The resultant accumulation of metformin may result in the development of the potentially fatal complication lactic acidosis.
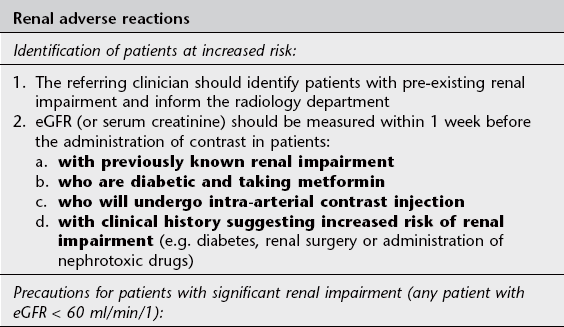
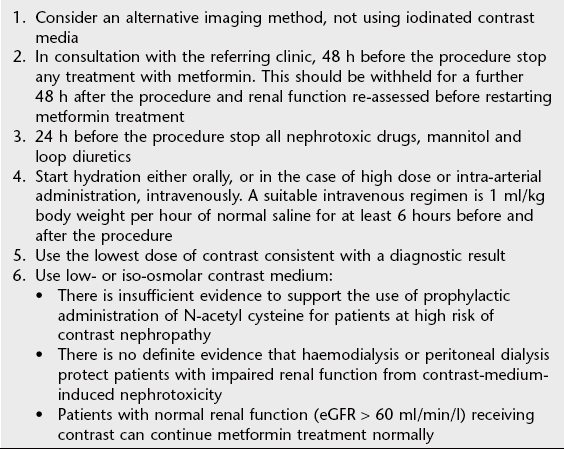
See Table 2.2 for guidelines on prophylaxis of renal adverse reaction to iodinated contrast.
Neurotoxicity
Contrast medium delivered to the brain via the arterial route during angiography or neurovascular intervention may rarely cross the blood–brain barrier with resultant cerebral oedema and altered neuronal excitability. Potential clinical effects include encephalopathy, seizures, cortical blindness and focal neurological deficits which are most often temporary but infrequently persistent.10 Neurotoxicity is caused by both osmolality and chemotoxic effects.
Intravenous contrast medium may rarely provoke convulsions in patients with epilepsy or cerebral tumours.
Convulsions may also occur secondary to the cerebral hypoxia caused by hypotension ± cardiac arrest after severe contrast reaction.
Thyroid function
1. Iodinated contrast media may rarely cause thyroid dysfunction resulting in the development of either incident hyperthyroidism or incident overt hypothyroidism.11 Iodide administration may result in the generation of intrathyroidal iodolactones or iodolipids which inhibit thyroid peroxidise activity and disrupt normal thyroid function. Patients with no known risk factors may be affected but those with goitre or proven detectable serum antibodies to thyroperoxidase are likely at increased risk, particularly in iodine-deficient geographic regions.
2. Contrast media may interfere with the accuracy of thyroid function tests.
Idiosyncratic reactions
Adverse reactions can be classified in terms of severity as:
1. Mild: Nausea, vomiting, urticaria
2. Moderate: Mild bronchospasm, vasovagal reaction, tachycardia, diffuse erythema
3. Severe: Cardiovascular collapse, moderate or severe bronchospasm, laryngeal oedema, loss of consciousness or seizure.
Mild and moderate reactions are uncommon; major adverse reactions are very rare for both LOCM12 and iso-osmolar iodinated contrast.13 Adverse effects of low osmolar iodinated contrast are found in approximately 0.15% of all patients. In a large study of LOCM contrast doses14 the adverse effects were categorized (Table 2.3).
Table 2.3
Categories of adverse effects of LOCM contrast doses14
| Category of adverse effect14 | Proportion of adverse effect events (n = 458) | Proportion of total patient group (n = 298 000) |
| Mild | 81.6% | 0.125% |
| Moderate | 15.1% | 0.02% |
| Severe | 3.3% | 0.005% |
The vast majority of adverse effects were managed with patient re-assurance or diphenydramine treatment and one death was presumed caused by LOCM (0.0003% of total patient group).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


