Intravascular ultrasound (IVUS) has become an essential tool for endovascular procedures, particularly during complex interventions. The benefits include improved visualization of vascular and extravascular anatomy, reduced complication rates, and enhanced accuracy during catheter-based interventions. In this review, we discuss the properties of side-firing (also commonly known as intracardiac echo ICE) and radial IVUS and explore their unique applications in endovascular procedures. The side-firing IVUS is advantageous for visualizing lesions and vascular structures in a plane parallel to the vessel wall, making it effective for guiding portal venous interventions, transvenous biopsies, and endoleak embolization, while the radial IVUS provides a 360-degree view of the vessel lumen, enabling detailed cross-sectional images of normal anatomy, pathologic processes requiring different endovascular therapy and their response to intervention(s).
Introduction
Intravascular ultrasound (IVUS) has become an extremely invaluable endovascular evaluation tool that offers comprehensive assessments of vascular conditions and perivascular anatomy, providing critical information that enhances clinical decision-making. The benefits include improved visualization of vascular and extravascular anatomy leading to reduced procedure times, complication rates, and enhanced accuracy during catheter-based interventions. There are 2 types of IVUS available currently—radial and side-firing. The radial IVUS provides a 360-degree view of the vessel lumen, whereas the side-firing IVUS allows visualization of vascular and extravascular structures in a plane parallel to the vessel wall.
Radial IVUS is primarily used to determine the vessel size, severity and length of stenosis and plaque composition, as well as to detect pathological processes such as plaque rupture and dissections. Another significant advantage is its ability to confirm the position of intravascular devices, ensuring true lumen access versus a false lumen during endovascular interventions. It also allows identifying the origins of side branches without needing contrast materials, which can be critical for therapeutic interventions. Moreover, it can be utilized to assess extrinsic venous compression, identifying potential impacts from surrounding structures. Finally, IVUS is instrumental in evaluating the completeness and response to treatment, allowing proceduralists to verify the effectiveness of procedures such as stenting or angioplasty, thereby ensuring optimal treatment outcomes. The side-firing IVUS has been historically used for intracardiac echocardiography for trans-septal puncture, left atrial appendage closure, and intracardiac biopsies but has recently gained popularity for interventional radiological procedures such as trans jugular intrahepatic portosystemic shunt placement (TIPS), transvenous biopsies and transcaval abdominal aortic aneurysm endoleak embolizations. ,
Overall, the insights gained from IVUS are invaluable in guiding and optimizing endovascular interventions. In the current review, we will compare the different IVUS modalities, discuss their different clinical applications and review basic techniques.
IVUS catheters
The available radial IVUS catheters feature radially arranged transducer elements with an integrated circuit near the tip of the catheter. Radial IVUS catheters are designed to provide detailed, high-resolution, cross-sectional images of blood vessels. Higher ultrasound frequencies result in shorter wavelengths, which enhance detail and spatial resolution but sacrifice penetration depth. Remember that axial resolution in ultrasound is calculated as half the spatial pulse length. The radial IVUS catheters are currently available in 0.014, 0.018, and 0.035 systems.
The available 0.014 catheters include the Opticross HD (Boston Scientific, Marlborough, MA), which is available in 3.1 French diameter, operates at a frequency of 60 MHz and has a maximum imaging diameter of 6 mm. The Visions PV RX 0.014 (Philips, Andover, MA) is available in 3.5 French, operates at 20 MHz, and has a maximum imaging diameter of 20 mm. The Pioneer Plus (Philips) is a 0.014 compatible rapid exchange radial IVUS guided reentry catheter that operates at 20 MHz; it features an adjustable 24-gauge reentry needle with needle throws available at 3 mm, 5 mm, or 7 mm and supports a maximum imaging diameter of 20 mm. This catheter also includes color Doppler functionality.
The available 0.018 catheters include the Visions PV RX .018 and the Reconnaissance PV .018 OTW (Philips, Andover, MA), available in 3.5 French, operating at a frequency of 20 MHz. While the maximum imaging diameter for Vision PV is 24 mm, the Reconnaissance PV .018 has a slight reduced imaging diameter of 20 mm. Both the .014 and .018 Vision PV RX catheters are equipped with color Doppler functionality.
For the 0.035 category, the Visions PV .035 (Philips, Andover, MA) is available in 8.2 French operating at 10 MHz, with a maximum imaging diameter of 60 mm. The OptiCross 35 (Boston Scientific, Marlborough, MA), is available in 8 French, operating at 15 MHz, with a maximum imaging diameter of 70 mm. Notably, The Visions PV features 25 radiopaque markers along the catheter shaft, spaced 1 cm apart, which can helpful to plan endovascular interventions. All of the above 0.035 catheters and the Reconnaissance PV .018 OTW are over-the-wire catheters, while the other catheters are monorail systems designed for rapid exchange.
In contrast, the side-firing IVUS is a lower-frequency phased-array side-firing probe that generates a 90° field of view, allowing for greater tissue penetration due to its reduced frequency. Several side firing IVUS catheters are available commercially including Abbot/St Jude Medical, Philips, GE Health Care and Siemens and authors recommend checking compatibility of the available ultrasound consoles with side firing IVUS probe prior to use. The authors have discussed the most frequently used side firing IVUS probes below.
The ACUSON AcuNav (Siemens Healthineers) features a 64-element phased-array design with a side-firing configuration. It operates at frequencies between 5 and 10 MHz, providing longitudinal single-plane imaging, a 90° field of view, and Doppler capability, with penetration depths reaching up to 16 cm and are available in 8 Fr and 10 Fr diameter. It is equipped with steering control knobs that enables maneuvering the catheter in 2 directions: left/right and anterior/posterior.
Similarly, the ViewFlex Xtra (Abbot / St. Jude Medical) is a 64-element phased-array side-firing probe, boasting a diameter of 9 French (compatible with a 10 Fr sheath). It functions at frequencies from 4.5 to 8.5 MHz and achieves penetration depths of up to 21 cm. The Verisight Pro (Philips, Andover, MA) is a 9F catheter with a broad range of frequencies from 4 MHz to 10 MHz, 3D capability, and allows 4 ways of deflection. In contrast to the radial IVUS, none of these catheters operate over the wire and must be unsheathed directly within the vessel.
Clinical applications of radial IVUS
Peripheral arterial disease
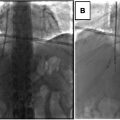
Radial IVUS has proved to be an extremely invaluable tool in peripheral artery disease intervention. It helps evaluate the trilaminar structure of the artery, with the intima and adventitia appearing hyperechoic, while the media is seen as hypo/isoechoic. It allows for the accurate measurement of the cross-sectional area of the vessel and has proved to be more precise in measuring the lumen size and percent stenosis compared to angiography. This improved accuracy can result in better sizing of devices for endovascular therapies, such as balloons and stents. In a study focused on the infra-popliteal arteries, the use of IVUS led to the selection of larger balloon sizes for interventions; the IVUS group had better skin perfusion and wound healing outcomes compared to the angiography-only group. After stent deployment, IVUS can uncover insufficient apposition or under-expansion of stents. Moreover, IVUS can differentiate the true and false lumens for ensuring optimal outcomes in stenting and reconstruction procedures ( Fig. 1 ).

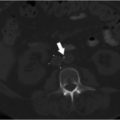
Additionally, the distinct capability of IVUS to evaluate plaque composition and morphology can assist in determining the appropriate vessel preparation strategies. Generally, soft plaque has echogenicity lower than that of the adventitia, while fibrotic plaque displays echogenicity equal to that of the adventitia. In contrast, calcified plaque presents with echogenicity greater than that of the adventitia and may demonstrate posterior acoustic shadowing. Mixed plaque contains a combination of soft, fibrotic, and calcified components, resulting in varying echogenicities ( Fig. 2 ). A retrospective study evaluated the outcomes of IVUS compared to angiography guidance for directional atherectomy in revascularization for femoropopliteal intrastent stenosis, revealing better results in the IVUS group, which had fewer clinically driven target lesion revascularizations. IVUS imaging was more effective at identifying dissections than angiography, however clinical significance of this increased sensitivity in dissection detection remains to be further investigated ( Fig. 3 ). The Peripheral Arterial Intervention Registry for Medicare patients found that the use of IVUS was linked to a reduced risk of major adverse limb events in both the short term and long term.