Various congenital anomalies of the pancreas have been described, which includes pancreas divisum, annular pancreas, ectopic pancreas, duplication anomalies, variations in the course of pancreatic duct, dorsal agenesis and intrapancreatic accessory spleen.
Index case: A 53-year-old female presented with on and off pain abdomen.
Radiological technique: Magnetic resonance cholangiopancreatography (MRCP).
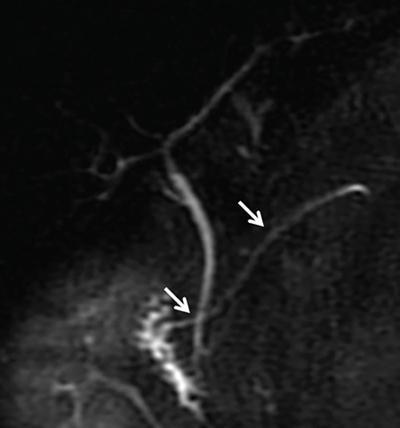
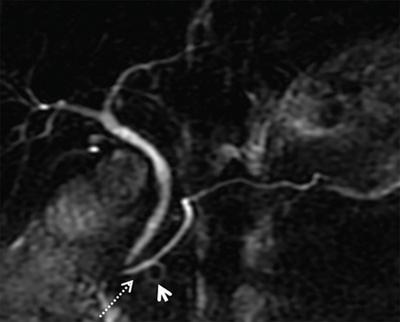
Observations: MRCP image showing the dominant dorsal duct of Santorini (arrows) draining separately into the minor papilla. The common bile duct (CBD) is joining the smaller ventral pancreatic duct through the major papilla.
Principal diagnosis: Pancreas divisum.
Differential Diagnosis for Congenital Pancreatic Anomalies
Diagnosis
Imaging Features
Images
Pancreas divisum
• Seen in 4%–14% of the population.
• Three variants have been described: Total failure of fusion (type 1), dorsal drainage is dominant with the absence of the duct of Wirsung (type 2) and incomplete divisum with small communicating branch (type 3).
• Due to the inadequate drainage of pancreatic secretions via the minor papilla, patients usually present with recurrent attacks of pancreatitis.
Congenital variations of the pancreatic duct
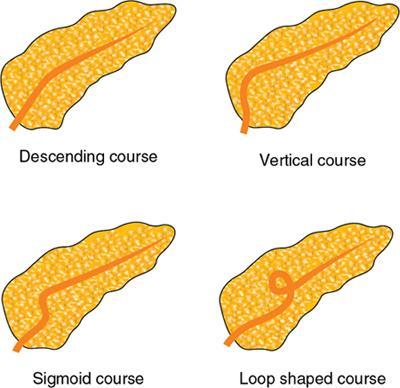
Variations in the course of pancreatic duct – descending course, vertical course, sigmoid course and loop-shaped course.
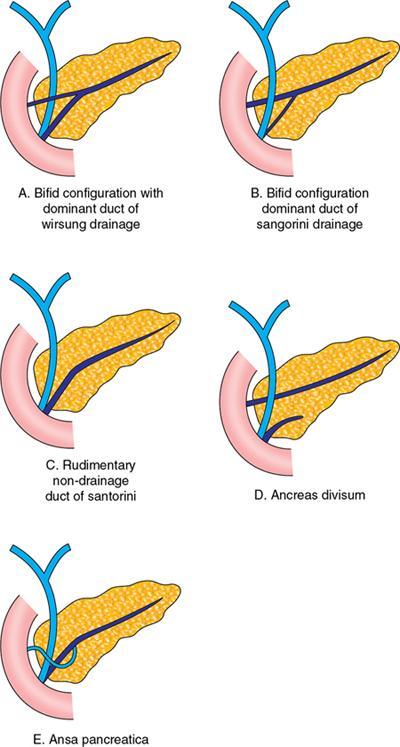
Variation in the configuration of pancreatic duct – dominant duct of Wirsung drainage, dominant duct of Santorini without divisum, pancreas divisum and ansa pancreatica.
Variations in the course of pancreatic duct.
Variation in configuration of pancreatic duct.
Ansa pancreatica
Ansa pancreatica is seen when there is obliteration of the dorsal pancreatic duct at the junction with ventral duct, and instead, the proximal portion of the dorsal duct connects with an inferior side branch of the ventral duct through an S-shaped collateral duct.
MRCP image of ansa pancreatica in a 43-year-old male. The proximal dorsal duct connects with an inferior branch of the ventral duct (dashed arrow) through S-shaped collateral. (arrowhead)
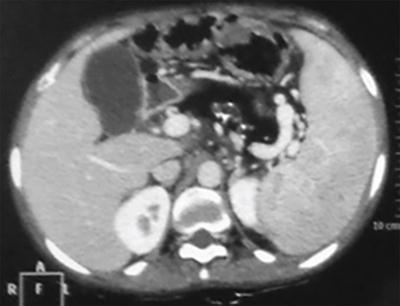
Annular pancreas
• There are two types of annular pancreas: Extramural and intramural. In the extramural type, the ventral pancreatic duct encircles the duodenum to join the main pancreatic duct. In the intramural type, the pancreatic tissue is intermingled with muscle fibres in the duodenal wall, and small ducts drain directly into the duodenum.
• At CT MRI, a ring of pancreatic tissue surrounds the descending duodenum, in continuity with the pancreatic head.
• Rim of pancreas in anterior or posterior aspect forming ‘crocodile jaw configuration’ should raise the suspicion of annular pancreas.
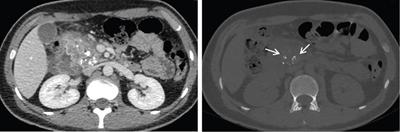
Axial CT image shows pancreatic tissue (arrows) completely encircling the second part of the duodenum in patient with extramural annular pancreas.
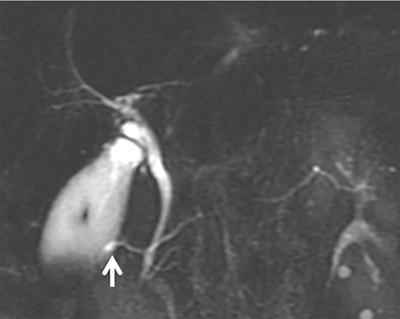
Santorinicele and Wirsungocele
• Cystic dilatation of the distal dorsal duct, just proximal to the minor papilla, is termed as Santorinicele. And, cystic dilation of terminal ventral pancreatic duct (Wirsung’s duct) is known as Wirsungocele.
• Santorinicele has been associated with pancreas divisum and is associated with recurrent pancreatitis.
• Wirsungocele has recently been shown to be associated with acute recurrent, severe necrotizing pancreatitis and chronic pain in abdomen.
2D MRCP image showing the pancreas is being drained by the dominant dorsal duct, which is crossing the CBD and draining at the minor duodenal papilla. In addition, there is focal dilatation (arrow) of the dorsal duct near the papilla consistent with Santorinicele.
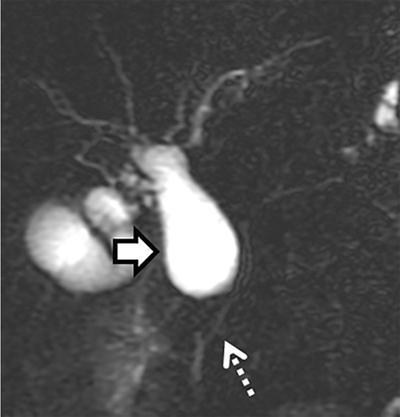
Anomalous pancreaticobiliary junction (APBJ)
• APBJ refers to anomalous union of the pancreatic and bile ducts outside the duodenal wall resulting in a long common channel, which is more than 15 mm.
• Associations of APBJ: Pancreatitis, gallbladder cancer and cholangiocarcinoma.
2D MRCP image showing congenital choledochal cyst (arrow) with a long common channel (dashed arrow) joining the CBD.
Dorsal agenesis
• Complete agenesis is extremely rare and is characterized by complete absence of the neck, the body and the tail of the pancreas along with missing accessory duct of Santorini and minor papilla.
• In partial agenesis, the pancreatic body is of variable size, a remnant of the accessory duct of Santorini exists and the minor papilla is present.
• Fifty per cent of patients with dorsal agenesis manifest as hyperglycaemia.
• On imaging, absent pancreatic tissue ventral to the splenic vein with abrupt truncation is seen.
• It is important to differentiate pancreatic agenesis from atrophy and lipomatous replacement of the pancreas. Dependent stomach and/or dependent intestine signs are helpful in differentiating dorsal agenesis from distal lipomatosis.
• In the dependent stomach or dependent intestine sign, the pancreatic bed is occupied by stomach or intestine abutting the splenic vein. In lipomatosis, abundant fat is observed anterior to the splenic vein.
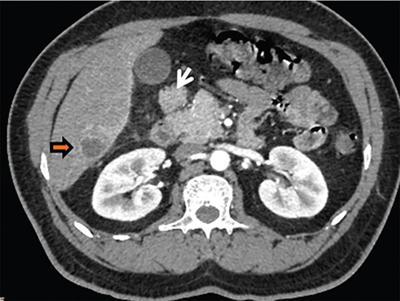
Axial contrast-enhanced computed tomography (CECT) image showing short truncated pancreas with the absence of body and tail of pancreas. Small intestinal loops are seen in the pancreatic bed suggestive of dorsal pancreatic agenesis.
Axial CECT images showing fatty replacement of pancreas with intraductal calculi in a known case of cystic fibrosis.
Intrapancreatic accessory spleen
• Accessory splenic tissue may be located in the body–tail region of the pancreas, mimicking an infiltrative process such as autoimmune pancreatitis or neoplasm, especially a pancreatic endocrine tumour.
• This entity can generally be recognized at multiphasic CT, since the tissue follows the enhancement pattern of the spleen.
Axial CECT image showing nodular accessory spleen (arrows) within the pancreatic tail having attenuation and enhancement similar to spleen on the arterial and the venous phase scans.
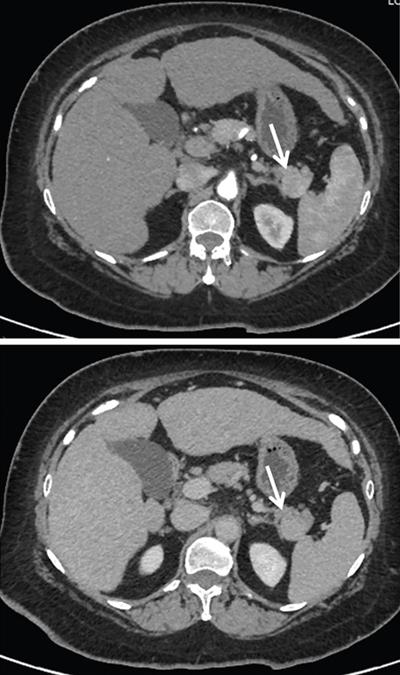
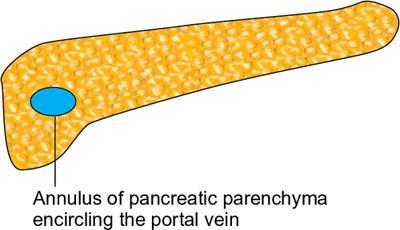
Circumportal pancreas
• Circumportal pancreas, refers to encirclement of the portal vein or superior mesenteric vein by an annulus of pancreatic parenchyma.
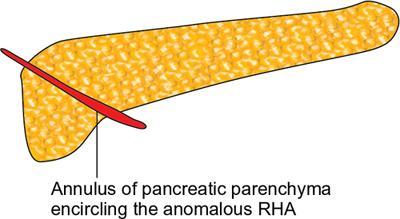
• Arterial annular pancreas is an uncommon variant wherein the pancreatic parenchyma encircles an anomalous artery, most commonly replaced right hepatic artery.
Ectopic pancreas
• The ectopic pancreatic tissue can be found in the stomach (26%–38%), duodenum (28%–36%), jejunum (16%), Meckel’s diverticulum or ileum. The size of ectopic pancreatic tissue is usually 0.5–2 cm.
Axial CECT image showing ectopic pancreatic tissue (arrow) with enhancement similar to main pancreatic parenchyma. Incidental note is made of small abscess (yellow arrow) in the liver.
Congenital pancreatic cysts
• Solitary congenital cysts of the pancreas are rare.
• Syndromes associated with cysts – von Hippel–Lindau (VHL) disease, cystic fibrosis, autosomal dominant polycystic kidney disease (ADPKD).
Axial CECT image showing complete replacement of pancreas with multiple cysts in keeping with pancreatic cystosis in a case of VHL.
Bifid tail of pancreas
• Bifid tail of the pancreas is a benign congenital variant. The clinical effect and importance of this anomaly remains uncertain.
• On MRCP or endoscopic retrograde cholangiopancreatography (ERCP), it manifests as duplication of the major duct in the body or tail of the pancreas.
Axial 3D MRCP image depicting bifid pancreatic duct in body region of pancreas (arrows) with changes of moderate to severe pancreatitis in the tail region (dashed arrow) in the form of dilated side duct branches.
9.4.2
APPROACH TO PANCREATIC CALCIFICATION
Binit Sureka, M.K. Mittal
Introduction
Pancreatic calcifications are key features commonly used to diagnose various types of pancreatic diseases. Awareness of these entities and classic features is important in making the correct diagnosis and guiding proper management.
Index case: A 19-year-old male, diagnosed case of cystic fibrosis presenting with recurrent episodes of pain abdomen.
Radiological technique
Contrast-enhanced CT (CECT) abdomen.
Observations
Bulky pancreatic head with adjacent duodenal wall thickening, minimal peripancreatic fat stranding with specks of calcification. Bone window showing central lucency within the calcification giving bull’s eye appearance. No vascular invasion/involvement. Retropancreatic fat planes preserved.
Principal diagnosis
Genetic mutation-associated pancreatitis.
Case of Genetic-mutation associated pancreatitis showing bull’s eye calcification.
Only gold members can continue reading. Log In or Register to continue