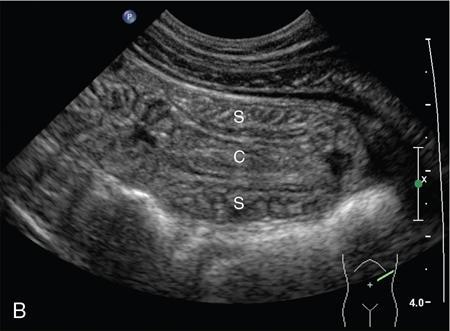
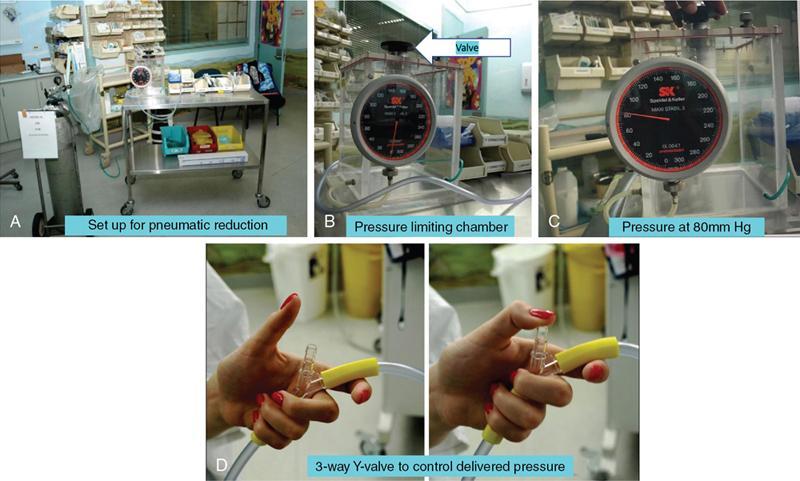
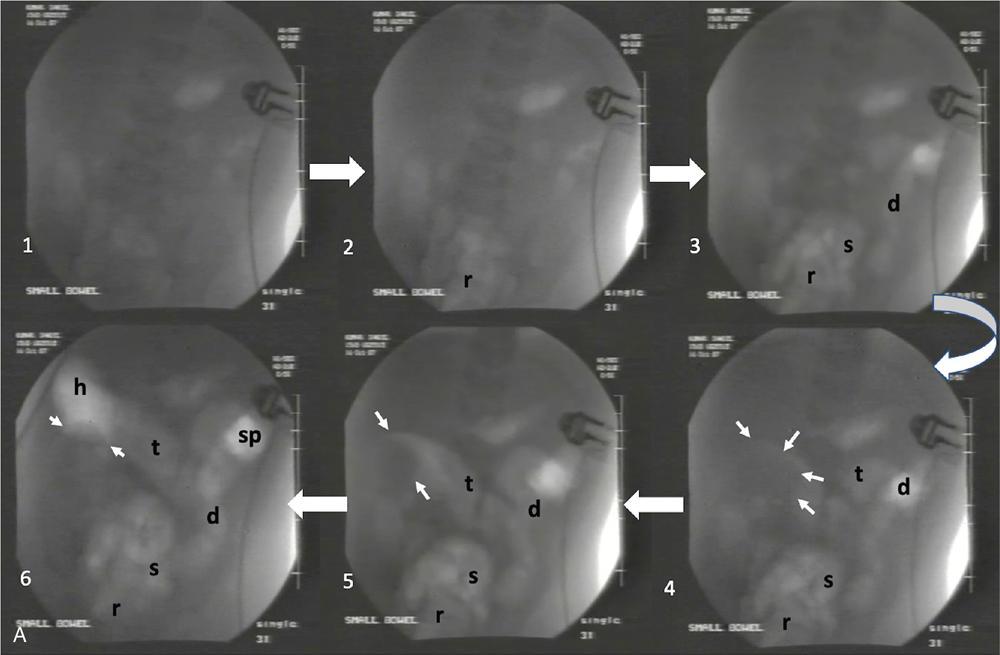
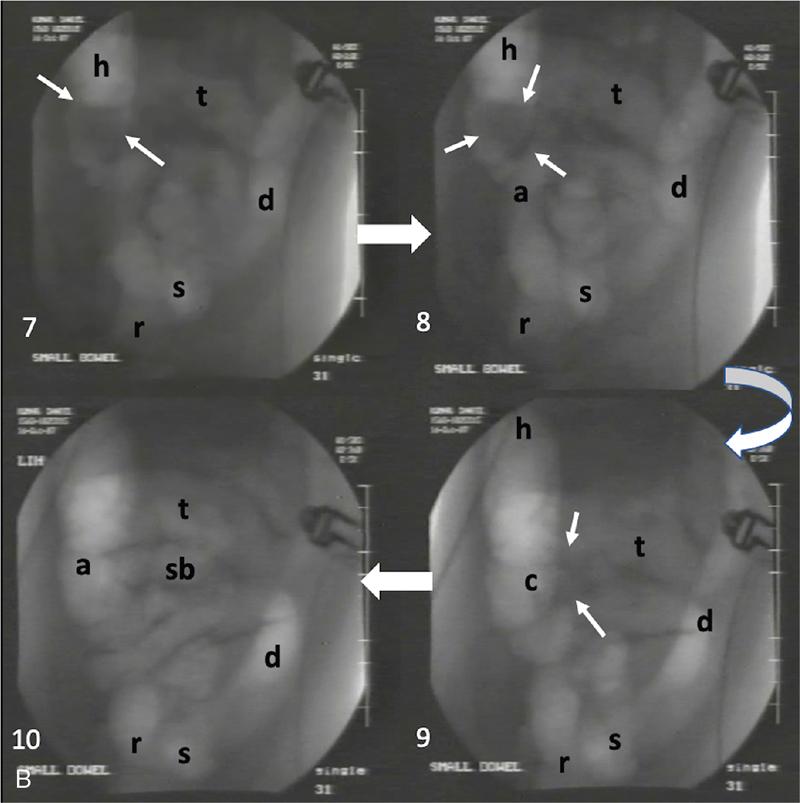
Ajay Taranath, Lino Piotto Intussusception is a common cause of acute abdominal pain in children. In this condition, a portion of the bowel wall, the intussusceptum, invaginates into the lumen of the portion of the bowel immediately distal to it, the intussuscipiens. It occurs most commonly in the first two years of life but is sometimes seen in older children. Once the invagination process has begun, the first part of the intussusceptum (the head) is pushed distally by peristalsis dragging the wall of the bowel with it. This tends to be progressive once it starts and as the invagination continues, interference with the blood supply of the intussusceptum causes venous occlusion and subsequent mucosal congestion. In advanced cases, the vascular compromise may result in the passage of blood-stained mucus through the rectum (red-currant jelly). Intussusception may be idiopathic or may be due to a pathologic ‘lead point’ such as a Meckel’s diverticulum, duplication cyst or neoplastic mass within the bowel wall. Most patients under the age of 2 years are in the idiopathic group. These are thought to be associated with thickening of bowel wall caused by hyperplasia of Peyer’s patches in response to a recent viral infection. Pathologic lead points are much more common in patients older than 4 years. For this reason, the head of the intussusceptum in these patients should be scanned carefully for evidence of a lead point. Intussusception is usually described according to the bowel that is involved. Those involving only small bowel include jejuno-jejunal (jejunum into jejunum) and ileo-ileal (ileum into ileum), are often seen as an incidental finding in abdominal sonography and only infrequently require intervention, when they have caused a bowel obstruction (Fig. 7.12.1A and B). Those involving large bowel include ileo-colic (ileum into colon), ileo-ileo-colic (ileum into ileum and then into colon) and colo-colic (colon into colon) and almost always require intervention. The most common of these is the ileo-colic type, in which the terminal ileum invaginates the colon through the ileo-caecal valve. The longer the intussusception persists, the greater the likelihood of gut necrosis and the need for surgical resection. Typically, children with intussusception will present with some or all of the following clinical features: attacks of colic, vomiting, blood and mucus per rectum, palpable abdominal mass. The attacks of colic are often associated with drawing-up of the legs. The duration of symptoms is usually less than 48 hours. The peak incidence is around 18 months though it can occur in children as young as 5 months and as old as 15 years. Traditionally, children suspected of suffering from an ileo-colic intussusception would be investigated with supine, erect and occasionally prone plain radiographs. When the clinical suspicion was high, the only way to confirm or exclude the presence of an intussusception was to perform a barium enema. A hydrostatic reduction using barium would then be employed to reduce an ileo-colic intussusception if one was found. More recently, pneumatic reductions have become the method of choice in many departments; benefits of this method include excellent reduction results and less radiation exposure than a barium enema. Pneumatic reductions have also shown to have greater reduction success rates than with barium. However, depiction rates of a pathological lead point on air enema are poor. Navarro et al. demonstrated a depiction rate of 11% in their study. Miller et al. showed a slightly higher depiction rate of 16%. Also, it must be noted that a successful reduction by an air enema cannot exclude a pathological lead point. In particular, lesions within the small bowel can be overlooked. Reduction rates also diminish when a pathological lead point is involved. Navarro et al. achieved a reduction rate of 29% in children presenting with their first episode of intussusception resulting from a pathological lead point. The relatively high-radiation dose from enema reductions was a significant factor in the development of ultrasound techniques, initially used only to identify those patients who had intussusception and therefore required a reduction. As a natural progression, the use of ultrasound in some institutions has been extended to monitoring of the reduction procedure. It is very important that the patient is well hydrated. It would be beneficial to have an intravenous access in all the patients with ileo-colic intussusception needing a pneumatic reduction. Administration of antibiotics may need consideration to ward off complications that might arise if there was an inadvertent perforation. It would be helpful to administer analgesics in consultation with the surgical team to help obtain compliance. The paediatric surgeon is in attendance. An 18 g cannula is kept handy to release the free air if a perforation occurs during the attempted reduction. The setup for a pneumatic reduction of intussusception (Fig. 7.12.2) consists of the following: (i) A cylinder of sterile medical air. (ii) A tube that leads away from the cylinder to a pressure limiting chamber. It has a dial indicating the pressure and a valve at the top of the chamber that will open if the pressure attained intraluminally goes over what has been set. (iii) A tube leading from the pressure-limiting chamber to a Foley’s catheter that is placed in the rectum. (iv) A three-way Y-valve (that can be controlled by the operator’s thumb in case the pressure control needs to be achieved quickly) is interposed midway in the tube leading out of the pressure chamber. It is important to get a good seal at the rectum. The chamber pressure is set at 80 mm Hg at the start of the reduction. A thumb rule of 3 is followed in that if there is no success with reduction after employing a pressure of 80 mm Hg for 3 minutes, it is increased to 100 mm Hg for 3 minutes and if the operator is comfortable, to 110–120 mm Hg for 3 minutes. If reduction is not achieved, surgical intervention may need to be considered in consultation with the paediatric surgeons. The air insufflation is begun. Retrograde movement of the intussusceptum is tracked fluoroscopically. There may be a point when the intussusceptum reaches the ileo-caecal junction and fails to respond to the air insufflation. It would helpful for the patient as the ileo-colic intussusceptions without pathological lead points tend to reduce, albeit in a delayed manner. The procedure is concluded when the insufflated air enters the small bowel loops (Fig. 7.12.3A and B).
7.12: Intussusception
Introduction
Aetiopathogenesis

Clinical features
Barium and pneumatic reductions
Technique of fluoroscopy-guided pneumatic reduction
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


