7 Ischemic Changes
Avascular Necrosis of the Humeral Head
Definition
 Demarcated area of necrotic bone marrow, spongiosa, and cortex in the humeral head
Demarcated area of necrotic bone marrow, spongiosa, and cortex in the humeral head
Pathology
 Damaged vascularization (blood supply and drainage, vascular structures) impairs the oxygen supply and induces necrosis of the cellular structures
Damaged vascularization (blood supply and drainage, vascular structures) impairs the oxygen supply and induces necrosis of the cellular structures
Staging
 Stage 0:
Stage 0:
– Histologically small marrow necroses, plasmostasis
 Stage I:
Stage I:
– Reversible early stage
– Repair process
– Proliferation of fibrovascular tissue
 Stage II:
Stage II:
– Irreversible early stage
– Insufficient repair mechanism with marginal sclerosis
 Stage III:
Stage III:
– Subchondral fracture due to mechanical failure
– Collapse of subchondral bone
– Flattening of the humeral head
 Stage IV:
Stage IV:
– Secondary osteoarthritis
– Destructive changes
Causes:
 Underlying diseases
Underlying diseases
– Gaucher disease
– Caisson disease
– Hemoglobinopathies (sickle cell anemia)
– Ionizing radiation
– Systemic lupus erythematosus
– Hypercorticoidism (corticosteroid therapy)
 Risk factors
Risk factors
– Alcoholism
– Dyslipidosis
– Hyperuricemia
– Pancreatitis
– Pregnancy
Clinical Findings
 Nonspecific pain
Nonspecific pain
Diagnostic Evaluation

Recommended views
 Anteroposterior (AP)
Anteroposterior (AP)
 Axial
Axial
 Possibly in internal and external rotation
Possibly in internal and external rotation
 Possibly “outlet view”
Possibly “outlet view”
Findings
 Stage 0/I: Normal findings
Stage 0/I: Normal findings
 Stage II: Sclerotic rim, densities
Stage II: Sclerotic rim, densities
 Stage III: Flattening of the humeral head, crescent sign
Stage III: Flattening of the humeral head, crescent sign
 Stage IV: Collapse
Stage IV: Collapse
 (→ Supplementary method)
(→ Supplementary method)
Findings
 Exclusion of associated changes:
Exclusion of associated changes:
– Effusion
– Tendon lesion
 (→ Supplementary method)
(→ Supplementary method)
Recommended protocol
 Unenhanced axial sections
Unenhanced axial sections
 Bone window display
Bone window display
Findings
 Stage 0/I: Normal findings
Stage 0/I: Normal findings
 Stage II: Sclerotic demarcation of the lesion, irregular trabecular structure
Stage II: Sclerotic demarcation of the lesion, irregular trabecular structure
 Stage III: Fracture of the subchondral bone
Stage III: Fracture of the subchondral bone
 Stage IV: Deformed humeral head
Stage IV: Deformed humeral head

Indications
 Staging
Staging
 Quantification
Quantification
 Localization
Localization
 Prognostic statements
Prognostic statements
Recommended sections
 Coronal
Coronal
 Axial
Axial
 Possibly sagittal
Possibly sagittal
Recommended sequences
 T1-weighted spin-echo (SE)
T1-weighted spin-echo (SE)
 Turbo inversion recovery magnitude (TIRM) (or fast spin [echo] T2-weighted imaging [FS TT2 w])
Turbo inversion recovery magnitude (TIRM) (or fast spin [echo] T2-weighted imaging [FS TT2 w])
 Possibly application of contrast medium
Possibly application of contrast medium
Findings
 Signal intensity of the necrosis:
Signal intensity of the necrosis:
– Type A: Isointense with fat (T1 weighting: hyperintense; T2 weighting: intermediate signal intensity; fast spin [echo] T2-weighted [FS T2]/short time inversion recovery [STIR]: low signal intensity)
– Type B: T1 weighting and T2 weighting: hyperintense, hemorrhage
– Type C: fluid-intense signal pattern, cystic components; T1 weighting hypointense, T2 weighting hyperintense
– Type D: Extensive fibrosis, sclerosis; T1 weighting and T2 weighting hypointense
Goals of Imaging
 Determination of the extent of the necrosis
Determination of the extent of the necrosis
 Presence of a subchondral or osteochondral fracture
Presence of a subchondral or osteochondral fracture
 Detection of an associated edema or effusion
Detection of an associated edema or effusion
 Determination of secondary degenerative changes
Determination of secondary degenerative changes
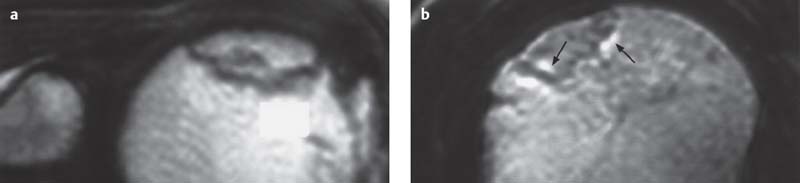
Fig. 7.1 a, b  Osteonecrosis, stage II
Osteonecrosis, stage II
a Sagittal T1-weighted SE sequence. Along the convex surface, a lesion separated from the remaining humeral head by a small signal-void rim (intact osteochondral interface).
b Coronal T2-weighted turbo spin-echo (TSE) sequence. The lesion is demarcated by a thin hypointense rim (sclerotic rim). Hyperintense signal changes are apparent along the lesion (granulation tissue, thin arrow), as well as along the adjoining bone marrow (discrete edema, curved arrow).
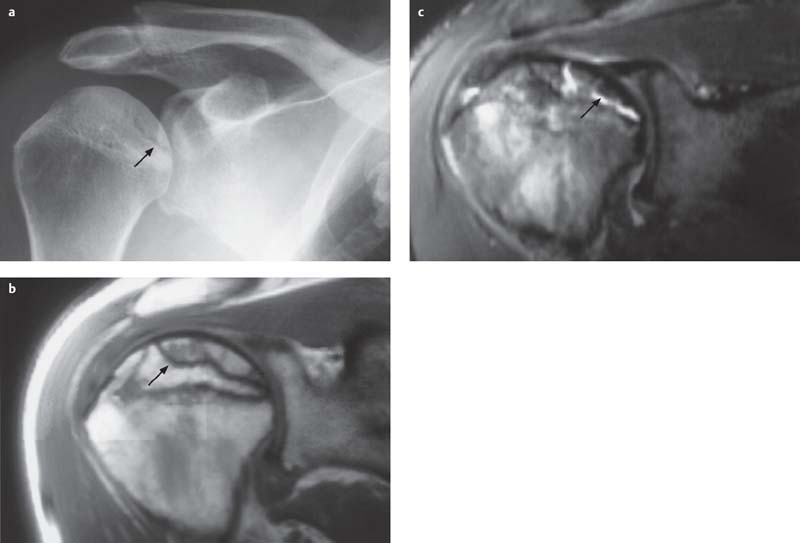
Fig. 7.2 a–c  Osteonecrosis, stage III
Osteonecrosis, stage III
a Conventional radiograph: The humeral head shows a small lesion, which is partially demarcated by a discrete radiolucent rim (subchondral fracture, arrow).
b
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


