10.12: Kidney
CYSTIC DISEASES OF KIDNEY
Vijay Kubihal, Chandan J. Das
Introduction
Renal cysts are the common incidental imaging findings due to the widespread use of ultrasonography and cross-sectional imaging. Simple uncomplicated cysts are often easy to diagnose. However, the complex cysts may be difficult to characterize as benign or malignant on imaging. With increasing incidence of renal cell carcinoma (RCC), and cystic RCC accounting for 15% of RCC, there is a need for reliable imaging method to differentiate benign from malignant cystic lesion. In 1986, Bosniak proposed a classification system to guide the characterization and management of the cystic renal lesions, which was then updated in 2005 (Table 10.12.1.1). Although Bosniak classification was initially developed for CT, it is now being commonly applied for other imaging modalities including CEUS and MRI. Contrast enhancement is the most important criterion used to differentiate surgical (Category III and IV) versus nonsurgical lesions (Category I, II and IIF).
| Type | Morphology | Wall | Septa | Calcification | Enhancement | Management |
|---|---|---|---|---|---|---|
| I | Simple cyst | Hairline thin | Absent | Absent | Absent | No further management |
| II | Hairline thin | Few, hairline thin | Fine | No measurable enhancement | No further management | |
| IIF | Hairline thin | More than few, hairline thin | Thick or nodular | No measurable enhancement | Follow-up | |
| III | Intermediate morphology | Thick irregular | Thick irregular | Any | Measurable enhancement seen | Surgery |
| IV | Cyst with solid component | Any | Any | Any | Enhancing soft tissue nodule | Surgery |
Simple renal cyst (Bosniak category I)
Simple renal cysts are quite common incidental finding, more commonly seen in elderly population.
They are thought to arise from weakening of the basement membrane, involving distal convoluted tubule or collecting duct, which results in formation of a diverticulum, and subsequently a cyst.
Simple renal cysts are usually asymptomatic, and incidentally detected, unless complicated. Complications include haemorrhage, infection, rupture, and caliceal or renal pelvic obstruction (Fig. 10.12.1.1).
- Imaging: Uncomplicated simple cysts are Bosniak type 1 cyst, characterized by thin hairline wall, and no septation, calcification or enhancement that are of water density (0–20 HU) on CT, and anechoic on USG.
- Renal sinus cysts are simple cysts that are present within renal sinus. It includes two distinct entity, namely, parapelvic cyst and peripelvic cyst. Parapelvic cyst is simple renal cyst that arises from medial renal parenchyma, and extends into renal pelvic sinus. These are usually asymptomatic. Sometimes, they can compress on renal pelvis or vasculature to cause hydronephrosis, hypertension or haematuria. Second entity is peripelvic cyst, which are benign extraparenchymal cysts that are located in renal sinus, and are thought to be of lymphatic origin. They are rarely symptomatic (Fig. 10.12.1.2).
- Renal sinus cyst could mimic hydronephrosis, that can be differentiated on excretory phase of CT urography, as these cysts do not show contrast opacification in excretory phase.
- Renal sinus cysts are simple cysts that are present within renal sinus. It includes two distinct entity, namely, parapelvic cyst and peripelvic cyst. Parapelvic cyst is simple renal cyst that arises from medial renal parenchyma, and extends into renal pelvic sinus. These are usually asymptomatic. Sometimes, they can compress on renal pelvis or vasculature to cause hydronephrosis, hypertension or haematuria. Second entity is peripelvic cyst, which are benign extraparenchymal cysts that are located in renal sinus, and are thought to be of lymphatic origin. They are rarely symptomatic (Fig. 10.12.1.2).
- Risk of malignancy: Simple renal cysts are benign finding with no risk of malignancy.
- Management: Simple renal cysts are left untreated unless symptomatic. Treatment options for symptomatic cysts include (1) simple aspiration, (2) aspiration with sclerosant injection, and (3) surgery (open, laparoscopic, or robotic). Rationale behind using sclerosant is to destroy the secreting epithelium in the cyst wall, with resultant decrease in high recurrence rate associated with simple aspiration. Ethanol in concentration of 95% or 99%, is the commonly used sclerosant. Volume of ethanol injected is usually the 20%–50% of cyst volume, with maximum dose of 75–200 mL. USG or CT guidance can be used depending on the feasibility. Complications include pain, fever, intracyst bleed and uncommonly extravasation, and systemic effects as alcohol intoxication and shock.
Bosniak category II
- Imaging: Bosniak type II cysts include (a) minimally complex cysts that may show few thin internal septations and/or fine calcifications without measurable enhancement; and (b) Well-defined homogeneous nonenhancing high-density cyst measuring ≤3 cm, and is not completely intrarenal (at least one-fourth of the cyst should be extrarenal) (Fig. 10.12.1.3).
- Risk of malignancy: Bosniak type II cysts are benign, with no chance of malignancy.
- Recommendations: No further evaluation required.
Bosniak category IIF
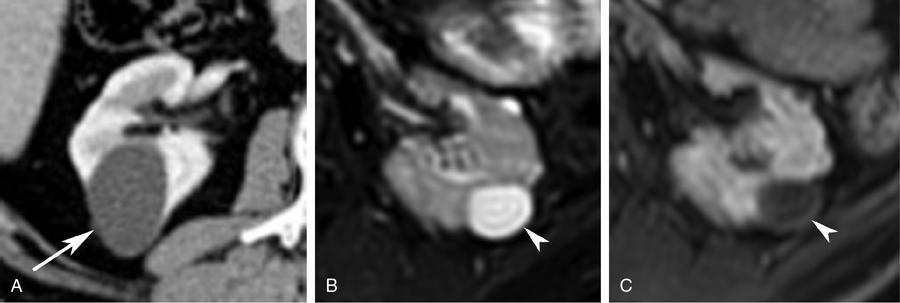
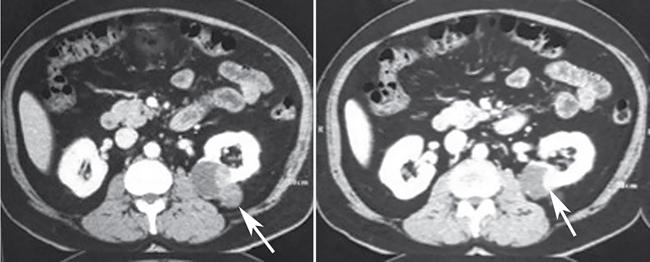
- Imaging: Bosniak type IIF cysts include (a) more complex cysts that may show more than few thin internal septations, minimally thickened septae and/or thick nodular calcifications without measurable enhancement; and (b) Well-defined homogeneous nonenhancing high-density cyst, either, measuring >3 cm, or is completely intrarenal (Fig. 10.12.1.4).
- Risk of malignancy: 5%.
- Recommendations: Follow-up with CT or MRI is recommended. Recommendation for duration of follow-up vary, ranging from 1 to 2 years, and sometimes more than 4 years, depending on complexity of the cyst.
Bosniak category III
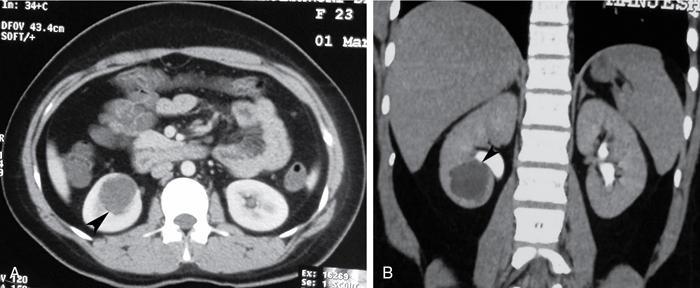
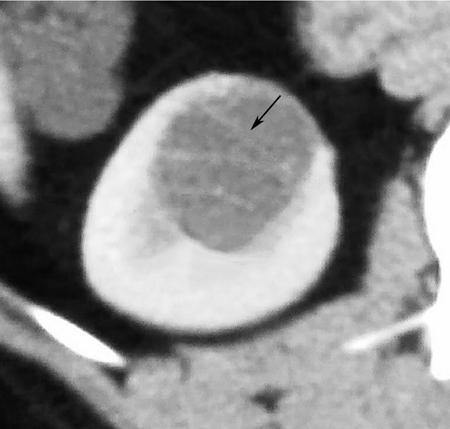
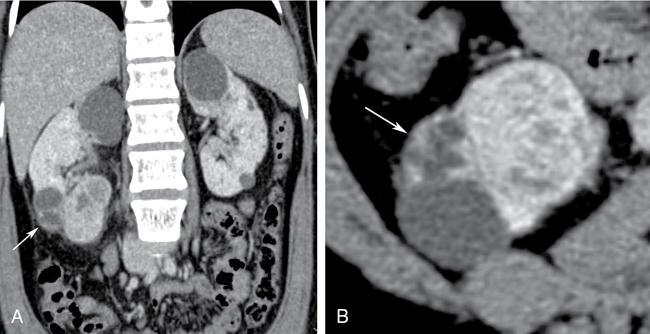
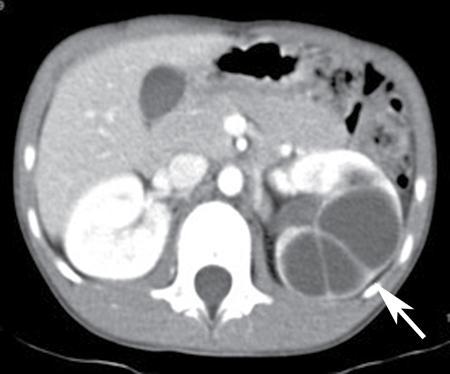
- Imaging: Bosniak type III cysts are indeterminate cystic masses with thick irregular wall or septae, showing measurable enhancement (Fig. 10.12.1.5). Apart from RCC, differential for Bosniak type III cysts are cystic nephroma (Fig. 10.12.1.6), benign multiloculated cyst, mixed epithelial and stromal tumour (MEST), renal abscess and haemorrhagic cyst.
- Risk of malignancy: 30%–100%.
- Recommendations: Biopsy carries increased risk of false-negative results due to small volume of tumour cells within the cyst. Thus, usual recommendation for type III cysts is surgical resection.
Bosniak category IV
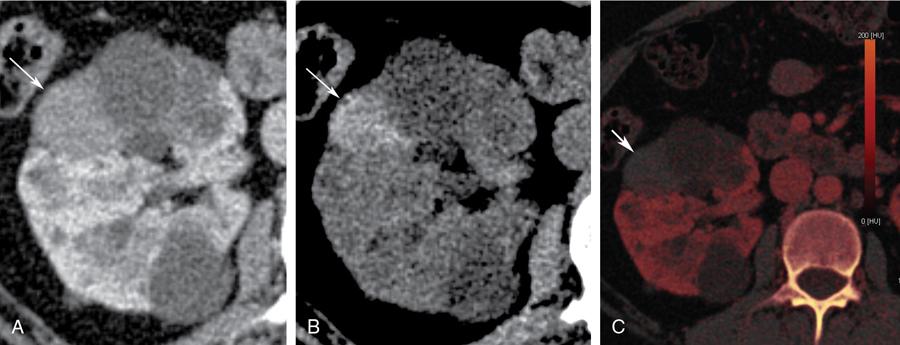
- Imaging: Bosniak type IV cysts are characterized by the presence of enhancing soft tissue nodule (Fig. 10.12.1.7).
- Risk of malignancy: They are considered malignant until proven otherwise, with risk of malignancy being 95%–100%. Very small percentage can be benign, example being MEST.
- Recommendations: Surgical resection is recommended if feasible.
2019 modification of Bosniak classification by Silverman et al.
Even though Bosniak classification is widely followed, there are certain limitations that include interreader variability, lack of clear definition of terms, variability in reported malignancy rates in individual Bosniak types, high prevalence of benign lesion in Bosniak type III cysts, and thus, increased surgery rates for benign cystic lesions. To address these limitations, modification to Bosniak classification was suggested by Silverman et al. (Tables 10.12.1.2 and 10.12.1.3), which requires further validation before wide spread use of it. Modified Bosniak classification described cystic mass as the one having ~<25% of enhancing soft tissue. Mass is considered enhancing, (a) if there is clearly visible enhancement, or (b) in case of not visibly enhancing mass, which is large enough to use conventional-sized regions of interest, shows measurable enhancement. Measurable enhancement is defined as increase of ≥20 HU on contrast-enhanced CT, or increase of ≥15% signal intensity on contrast enhancement MRI, compared to respective noncontrast images.









