| SKULL BASE REGION | Cerebellopontine angle/internal auditory canal |
| HISTOPATHOLOGY | Schwannoma |
| PRIOR SURGICAL RESECTION | Yes |
| PERTINENT LABORATORY FINDINGS | Pretreatment audiogram: Class A hearing bilaterally |
Case description
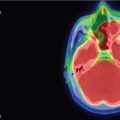
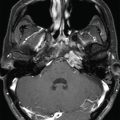
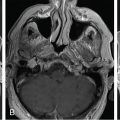
The patient presented at 35 years of age with significant incoordination while playing softball. She presented to a local otolaryngologist with symptoms of dysphagia and throat pain after accidentally colliding with a teammate, suffering a blunt injury to the neck. She was found to have edema in her pharynx and false vocal cords on direct laryngoscopy, and a computed tomography (CT) scan of the neck was obtained. A large right cerebellopontine angle (CPA) mass was incidentally captured on the scan, measuring 3.8 cm at its largest dimension ( Figure 8.38.1 ). There was associated mass effect on the pons and cerebellum without parenchymal edema or hydrocephalus. An audiogram was normal. She reported lightheadedness with changing positions but no real vertigo. She had no history of facial weakness or numbness. She did have a long-standing history of occipital headaches that radiated to the forehead, which is not typical of migraines. She had a normal neurological examination.

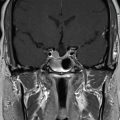
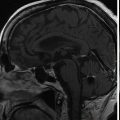
Due to the size of the lesion, she underwent a right retrosigmoid craniotomy for aggressive but subtotal resection to preserve the facial nerve. Unfortunately, hearing could not be preserved. The tumor was confirmed to be a schwannoma. Postoperative facial nerve function was House-Brackman (HB) grade 3 at worst but returned to normal by the 3-month follow-up. She developed worsening of her chronic headaches that required adjunctive medications. Postoperative magnetic resonance imaging (MRI) revealed a 9-mm plaque of tumor along the facial nerve ( Figure 8.38.2 ). She subsequently underwent “upfront” Gamma Knife radiosurgery (GKRS) to the residual tumor within 5 months of resection ( Figure 8.38.3 ).
| Radiosurgery Machine | Gamma Knife – Perfexion |
| Radiosurgery Dose (Gy) |
|
| Number of Fractions | 1 |

Related posts:
 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Suprasellar non-small cell lung carcinoma metastasis – upfront radiosurgery
Suprasellar non-small cell lung carcinoma metastasis – upfront radiosurgery
 Chondrosarcoma – definitive radiosurgery after subtotal resections
Chondrosarcoma – definitive radiosurgery after subtotal resections
 Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
 Capillary hemangioma – postoperative radiosurgery for residual tumor
Capillary hemangioma – postoperative radiosurgery for residual tumor
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


