LARYNGOCELE
KEY POINTS
- Computed tomography and magnetic resonance can confidently differentiate laryngoceles from other submucosal laryngeal masses and neck masses.
- Computed tomography can confidently but not entirely exclude an obstructing lesion, and magnetic resonance imaging is even less reliable in this matter.
INTRODUCTION
Etiology
Laryngoceles are lesions that arise spontaneously or due to obstruction of the saccule (appendix) of the laryngeal ventricle (Fig. 203.1). The presence of a laryngocele presupposes the presence of a saccule, which is not present in all patients.
Prevalence and Epidemiology
A laryngocele of the laryngeal ventricle saccule is a sporadic condition believed to be more frequent in wind instrument players or glassblowers (Fig. 9.17).
Clinical Presentation
Laryngoceles will most often present as a cause of laryngeal dysfunction, which on physical examination of the larynx will be accompanied by a submucosal mass. The dysfunction will manifest as dysphonia, airway obstruction, and/or swallowing problems. The other possible presentation is that of a neck mass typically bulging into the anterior triangle. About half of all submucosal laryngeal masses will be laryngoceles.
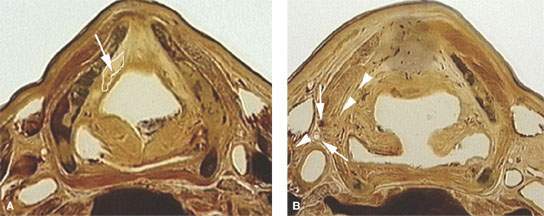
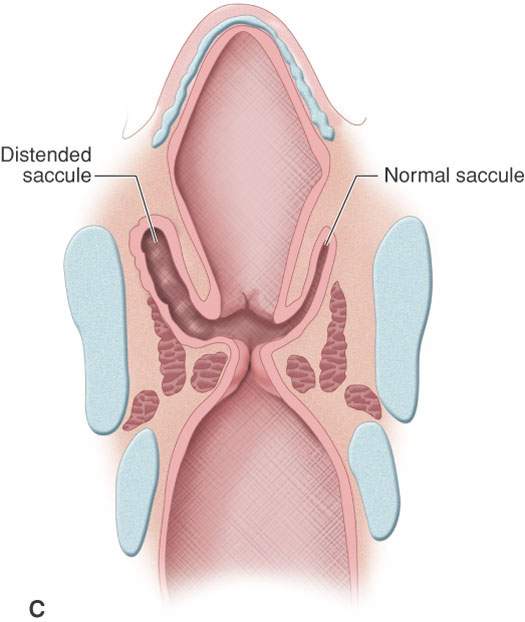
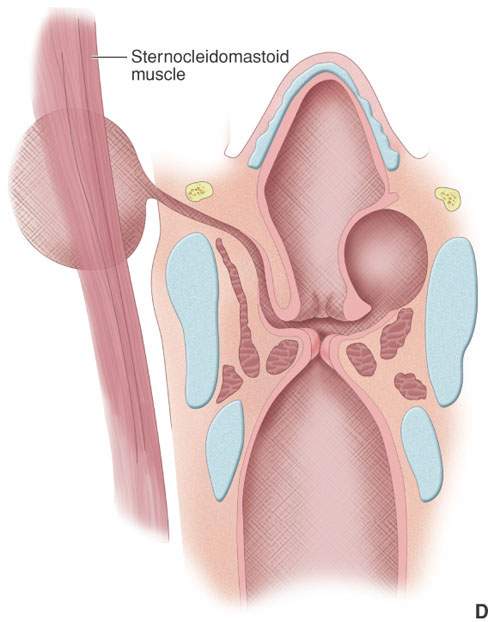
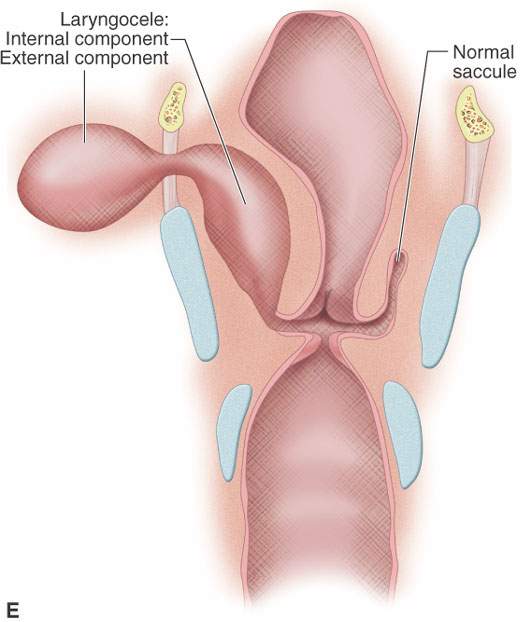
FIGURE 203.1. Anatomic diagrams to show the site of origin of laryngoceles and potential pathways of extension of internal, external, and combined laryngoceles. A: At the level of the false vocal cord, the position of the saccule (arrow at the collapsed saccule) that becomes distended by air and/or fluid to form a laryngocele. The white circle shows the general vicinity where the saccule may take its origin in the paraglottic space. B: Image taken through the mid supraglottic larynx showing how an internal laryngocele within the paraglottic space may extend toward the natural defect in the thyrohyoid membrane (arrowheads) that transmits the superior laryngeal neurovascular bundle (arrows). C: Distended saccule or early laryngocele compared to a normal saccule. D: Isolated internal and external laryngoceles. E: Combined laryngocele.
A clinical classification exists based on the location of the laryngocele. If the mass is entirely contained within the endolarynx, primarily in the false vocal fold and aryepiglottic fold, it is classified as internal (Figs. 203.2 and 203.3). An external laryngocele (Fig. 203.3) extends laterally superior to the superior border of the thyroid cartilage. Laryngoceles with components of both types are considered to be combined laryngoceles (Fig. 203.4).
If infected (a laryngopyocele), the mass may be tender and the patient may be febrile (Figs. 203.5 and 203.6).
The presence of a laryngocele requires a search for tumor obstructing the outlet of the saccule (Figs. 203.6 and 203.7).
PATHOPHYSIOLOGY
Anatomy
The laryngeal saccule is an oval air-filled structure that may be seen within the paraglottic space about one third of the way back from the anterior margin of the false vocal cord. Its size and shape varies. It may also be seen in its collapsed state as an obliquely oriented liner tissue density within the paraglottic fat medial to the lateral thyroarytenoid muscle. Sometimes it can be traced well superiorly within the anterior portion of the paraglottic space in either its slightly distended or nondistended state.
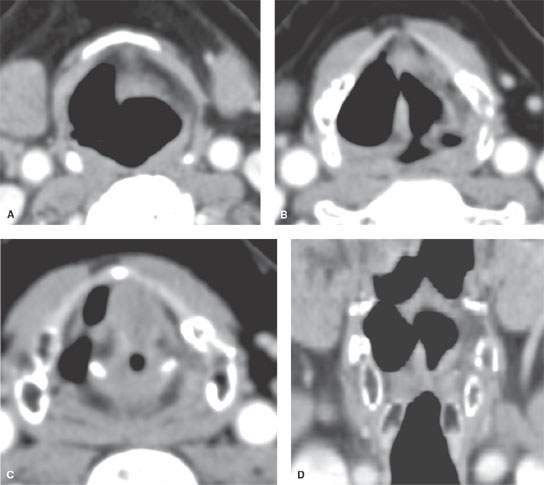
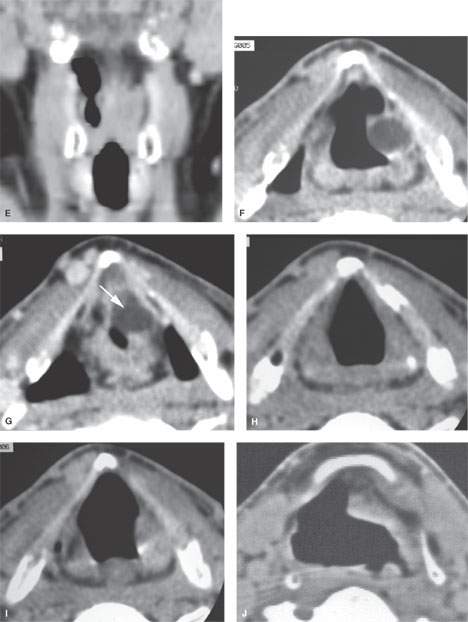
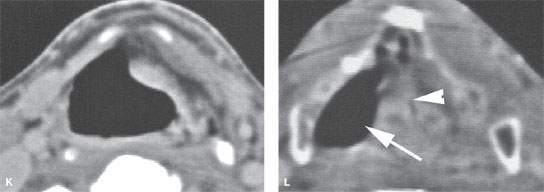
FIGURE 203.2. Computed tomography studies in three patients with various sizes and appearances of internal laryngocele. A–E: Patient 1 has an air-filled internal laryngocele that tracks from the supraglottic region inferiorly in the paraglottic space. The reformatted coronal sections in (D) and (E) show no evidence of an obstructing mass. (NOTE: Endoscopy showed no obstructing mass, and the laryngocele was presumed to be due to scarring or inflammation at the opening of the saccule.) F–I: Patient 2 presenting with a voice change and a submucosal mass at the level of the left false cord. The study shows a fluid-filled laryngocele limited to the left paraglottic space at the false cord level sections through the laryngeal ventricle in (H). In (I), there is no evidence of an obstructing mass. No mass was seen endoscopically. J, L: Patient 3 presenting with upper airway obstructive symptoms. This internal laryngocele actually trapped enough air that it encroached on the laryngeal vestibule and created upper airway obstruction. The laryngocele (arrow) can be seen at the false cord level in (I) compressing the false cords in the midline (arrowhead). (continued)
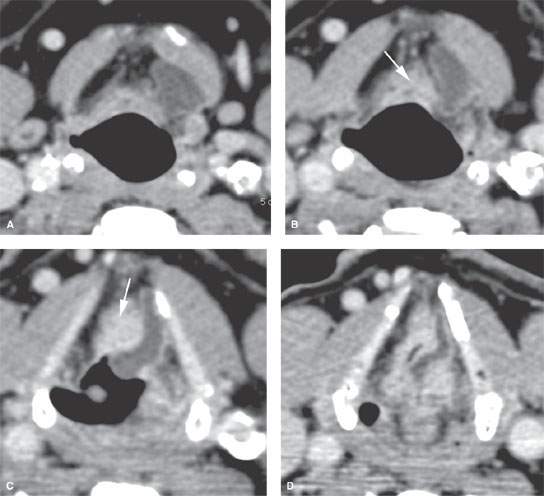
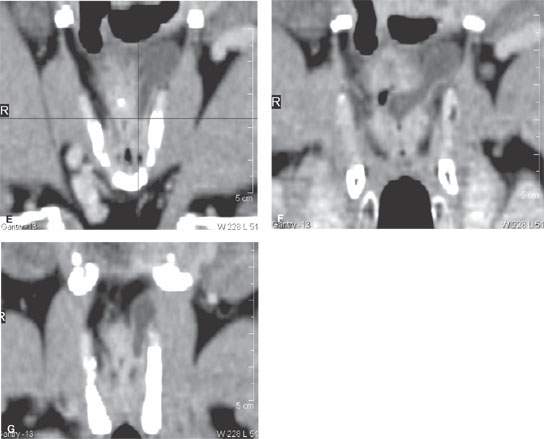
FIGURE 203.3. A patient with an internal laryngocele shown to be due to an obstructing tumor. In (A) and (B), the internal laryngocele can be seen tracking in the paraglottic space. In (C), enhancing tissue is present in the paraglottic and low pre-epiglottic space (arrows in B and C), with that tissue continuing to be visible at the false cord level in (D). The coronal sections in (E) through (G) show the fluid-filled obstructed saccule extending cephalad in the paraglottic space and bulging toward the thyrohyoid membrane. There is no external component. The enhancing mass is once again noted displaced slightly across the midline as seen in (E) through (G).
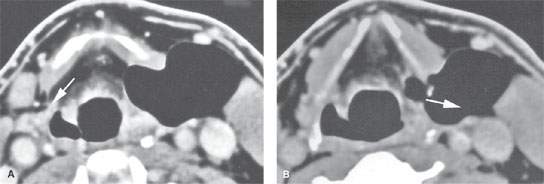
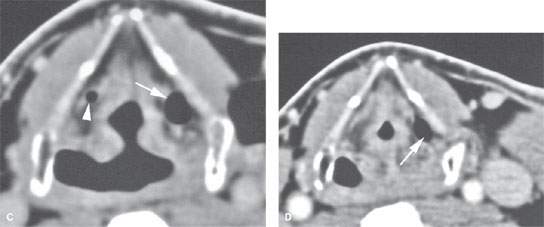
FIGURE 203.4. An example of an external laryngocele, which is an uncommon occurrence since a laryngocele is most commonly internal and, more occasionally, combined. In (A), the air-filled laryngocele bulges through the thyrohyoid membrane at the defect for the superior laryngeal neurovascular bundle (arrow on the normal side). Continuity between the distended saccule and the external laryngocele is shown by the arrow in (B). In (C), a slightly distended saccule is present on the left (arrow), and a normal air-filled saccule is seen on the right (arrowhead). The distended saccule is again seen in (D). (NOTE: Even an external laryngocele must have some connection to the saccule (appendix of the laryngeal ventricle) that is visible within the paraglottic space. If a cystic neck mass does not demonstrate such a connection to the saccule, then the diagnosis of a laryngocele is very unlikely.) (continued)
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Cervicothoracic Junction: Brachial Plexus Trauma
Cervicothoracic Junction: Brachial Plexus Trauma
 Oropharynx: Introduction
Oropharynx: Introduction
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


