LARYNX: DEVELOPMENTAL ABNORMALITIES
KEY POINTS
- Imaging may make a precise diagnosis in these anomalies.
- Imaging will significantly affect medical decision making in these developmental conditions.
- Computed tomography and/or magnetic resonance imaging are typically the main and frequently the only studies required.
- Ultrasound may be sufficient in the evaluation of simple abnormalities such as a noncomplicated thyroglossal cyst. However, in more complex problems, it will not provide information definitive enough for medical decision making.
Most congenital abnormalities of the larynx will not come to imaging. They will present as suggested subsequently and be evaluated clinically with direct endoscopy as directed by the clinical situation. Imaging only infrequently follows this initial clinical evaluation.
Congenital or early childhood vocal cord paralysis is not typically caused by a structural lesion, but it may come to imaging to exclude a mass compressing the vagus or recurrent laryngeal nerve or a clinically inapparent submucosal laryngeal mass mimicking cord paralysis as described in Chapter 138.
In general, developmental abnormalities of the larynx present during childhood. Some manifest in infancy; however, the presentation may be delayed until sometime beyond infancy well into the early adult years and even into middle age. If the lesion has growth potential, it tends to be at the same rate of normal structures, including a possible rapid growth phase at times of accelerated growth of the individual, such as adolescence. Some, such as high-flow vascular malformations, have internal physiologic dynamics that will allow them to enlarge more rapidly than normal tissues rather than truly proliferate. Truly neoplastic conditions such as a proliferative hemangioma (Chapters 8 and 9) will manifest growth out of proportion to normal structures.
Developmental abnormalities are frequently discovered incidentally on imaging studies done for other purposes. In the laryngeal-region lesion, this is most commonly due to a thyroglossal duct remnant. Some developmental conditions present as masses or because they interfere with function. In the larynx, they would typically manifest with dysphonia, aspiration, and/or airway symptoms. In an infant, airway problems are more likely and may manifest as sleep apnea. They are typically not painful unless there is some complicating factor. Developmental abnormalities may also manifest because of such complicating factors. Examples include infection in a cyst that connects to the pharynx; bleeding, thrombosis, or infection of a vascular malformation; or tumor arising in benign ectopic tissue, such as an adenoma or carcinoma in thyroglossal duct tissue.
The natural history and imaging appearance of the more common developmental abnormalities that affect the larynx primarily or secondarily are discussed in dedicated chapters on those topics as follows:
- Epidermoids, dermoids, and related abnormalities (Chapter 8)
- Thyroglossal duct abnormalities (Chapter 170)
- Branchial anomalies (Chapter 153)
- Vascular malformations (Chapter 9)
ANATOMIC AND DEVELOPMENTAL CONSIDERATIONS
Embryology
The embryology of the conditions that affect the larynx as presented in the introduction to this chapter is summarized in the dedicated chapters on those conditions as listed in the previous section.
A complete discussion of the cause of conditions typically evaluated by endoscopy, such as laryngeal clefts and webs, is beyond the scope of this text (Figs. 202.1 and 202.2). It is enough to understand that during the prenatal period, there is a time when the larynx must separate from the pharynx and then fuse its developmental elements in the midline. The separation process might be incomplete, leaving the two systems connected to some degree leading to a tracheoesophageal fistula. Failure of recanalization during this process may result in atresia, stenosis, or web formation in the larynx. Webs and the more severe anomalies typically will occur in areas that must separate side to side during development, such as the true vocal cords. Failure of obliteration can lead to a persistent posterior laryngeal cleft that causes aspiration in the newborn. Laryngeal agenesis may occur.
Applied Anatomy
A thorough knowledge of laryngeal anatomy and anatomic variations, as well as that of surrounding and otherwise related structures, is required for the evaluation of developmental conditions of the larynx. This anatomy is presented in detail with the introductory material on the larynx (Chapter 201), hypopharynx (Chapter 215), trachea (Chapter 209), cervical esophagus (Chapter 221), related spaces of the neck (Chapters 142 and 149), and oropharynx (Chapter 190).
IMAGING APPROACH
Techniques and Relevant Aspects
The larynx is studied in essentially the same manner for developmental abnormalities and other benign masses of known or uncertain etiology as it is for the evaluation of known or suspected laryngeal cancer. If a developmental defect is clearly suspected in a child, then intravenous contrast may not be necessary. The principles of using these studies are reviewed in Chapter 201. Specific problem-driven protocols for computed tomography (CT) and magnetic resonance imaging (MRI) of the larynx are presented in Appendixes A and B, respectively.
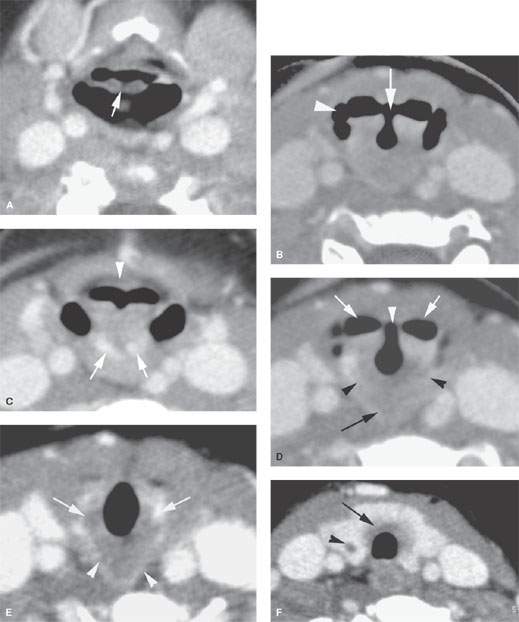
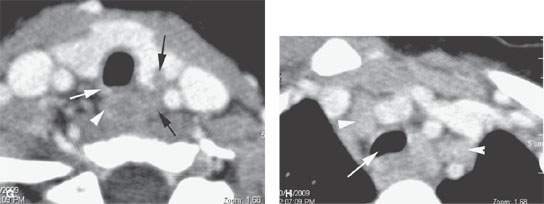
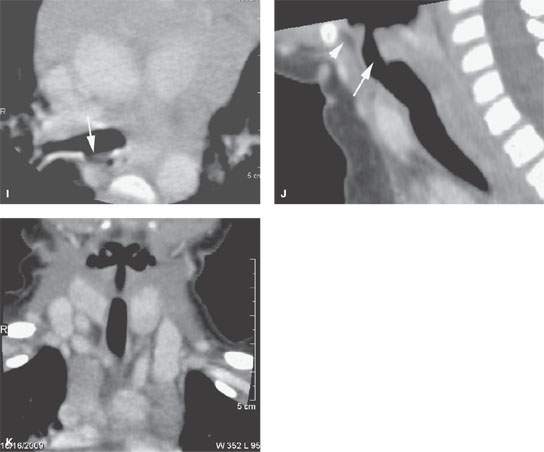
FIGURE 202.1. A 3 year old presenting with sleep apnea and a noisy upper airway. A computed tomography study with contrast shows what was believed radiographically to be a manifestation of cleft larynx. It was also considered suspicious for other associated anomalies. A: At the level of the suprahyoid epiglottis, there is a possibly unusual appearance of the free margin of the epiglottis (arrow). B: There is a dysmorphic-appearing laryngeal vestibule region (arrow) that has an unusual relationship with the pyriform sinuses (arrowhead). C: The densities seen posteriorly were presumed to be somewhat dysmorphic parts of the laryngeal skeleton, possibly the arytenoids (arrows). Also, there is a very shallow appearance of the pre-epiglottic space (arrowhead) and a somewhat unusual orientation of the aryepiglottic folds. D: At the level of the true vocal cords, there is an unusual relationship between the laryngeal vestibule and hypopharynx seen laterally and the glottic “chink” (white arrowhead). Black arrowheads show what appears to be portion of the cricoid cartilage and a somewhat dysmorphic-appearing postcricoid region. E: The dysmorphic postcricoid region (arrowheads) is seen to attach normally to the posterior aspect of the cricoid cartilage (arrows). F: An unusual amount of tissue lies between the thyroid gland and the first tracheal ring (arrow), and there is an abnormality in the thyroid gland possibly related to abnormal thymic tissue migration. G: The trend to possible associated thymic migration anomaly continues, where there is a cleft in the thyroid left lobe (black arrow). The relationship between the tracheal rings (arrow) and cervical esophagus (arrowhead) has returned to normal, distal to the unusual postcricoid region. H: There appears to be thymic tissue tracking on each side separately (arrowheads). The trachea is somewhat misshapen at the thoracic inlet. This might be a normal variant but suggests tracheal malacia. I: A small tracheoesophageal fistula was considered possible but was not confirmed at endoscopy. J: A sagittal reformation showing a very unusual appearance of the laryngeal vestibule (arrow) and a very small pre-epiglottic space. K: Coronal reformation showing the unusual relationship of the pharynx and laryngeal vestibule. (NOTE: By imaging, this study was felt to reflect anomalous development to the larynx within the spectrum of the laryngeal clefts. This was not specifically confirmed at endoscopy, although the larynx was noted to be somewhat unusual in appearance, and in this 3-year-old child, the glottis was said to have an “infantile” appearance. Despite the lack of specific endoscopic correlation, this larynx is clearly developmentally abnormal.
There is little or no use for ultrasound in studying these conditions, except for the in utero evaluation of fetal swallowing.
There is an extremely limited role for catheter angiography in lesions where the physical examination and imaging with CT angiography and/or MRI suggests that they are vascular in origin or very hypervascular.
Radionuclide studies are generally not useful in these conditions except to confirm the presence of ectopic thyroid tissue and confirm whether that ectopic tissue is the only functioning thyroid tissue present.

FIGURE 202.2. A 13-year-old patient suffering inspiratory stridor since birth, presenting with decreasing exercise tolerance. A coronal reformatted computed tomography image shows a subglottic web (arrows) narrowing the airway. The level of the true vocal cords is shown by the arrowheads. Laser resection of the web resulted in normalization of breathing.
Pros and Cons
In general, these anomalies occur in younger age groups, so it is best to avoid radiation if possible. On the other hand, definitive MRI in children may require general anesthesia. These relative risks must be balanced. Either MRI or CT may be definitive in the anatomic evaluation of these anomalies of development. CT generally will be more detailed, especially if information about the laryngeal skeleton is necessary for proper medical decision making; however, the laryngeal skeleton is not well mineralized until adulthood and is usually more difficult to see with CT in the young patient. One or the other may be more specific in some circumstances. MRI is more likely to be motion degraded, which may be particularly relevant when imaging small children.
Potentially developmental lesions that present as infections are better evaluated by CT. Such imaging is also more likely to show calcifications, if this is important for the differential diagnosis. MRI provides a better map of slow-flow venolymphatic malformations and can help to characterize cystic masses with diffusion-weighted imaging.
There really is no generally correct or incorrect choice in this matter. The decision of which imaging study to use should be individualized based on age, likelihood of the correct diagnosis already being known from clinical information, and availability of imaging equipment and other factors just discussed.
Controversies
It might be argued that ultrasound should be used in the evaluation of these problems, such as thyroglossal duct cysts. However, ultrasound is frequently not definitive and is cost additive, so its use as a “routine” seems unjustified. If it can truly obviate other more risky or expensive studies and provide all the information necessary for medical decision making, then it would be of obvious benefit in such an unusual circumstance.
SPECIFIC DISEASE/CONDITION
Developmental Cysts: Dermoid, Epidermoid, Duplication, Branchial Apparatus, and Thyroglossal Duct Cysts
Etiology
These anomalies are all spontaneous developmental abnormalities that only infrequently truly affect the larynx. Third branchial arch anomalies secondarily affect the larynx by way of a sinus tract present internally that pierces the thyrohyoid membrane (Fig. 153.15). This will connect to the pyriform and may become inflamed and cause laryngeal dysfunction. Infected cysts can also cause recurrent laryngeal nerve dysfunction, thus affecting the larynx secondarily. Duplication cysts of the larynx are very rare, likely appearing similar to bronchogenic cysts; it is very difficult to anticipate this diagnosis precisely prior to removal (Figs. 202.3 and 202.4).
The thyroglossal duct migrational abnormalities secondarily involve the larynx at the hyoid bone and occasionally by bulging into the supraglottic larynx.
Clinical Presentation
These anomalies will usually present as a palpable mass or because they interfere with the voice and airway function or cause aspiration in an adult. In an infant, these lesions may be detected by prenatal ultrasound but mainly will manifest at birth or shortly after birth as airway and/or feeding problems.
Branchial apparatus anomalies may present as an inflamed mid to low neck mass because they become infected or their tract to the pyriform sinus becomes obstructed1 (Fig. 153.15). They rarely present with abnormalities of swallowing in an adult or feeding in an infant associated with a submucosal mass, although the very rare duplication cyst can have this latter presentation.
Aberrant thyroid anomalies will usually present as a paramedian mass between the hyoid bone and lower margin thyroid notch; the mass may contain an adenoma or carcinoma and typically is not associated with any laryngeal or pharyngeal dysfunction or complaints. There may be pain or inflammation in this paramedian upper and mid neck mass caused by an infected thyroglossal duct cyst that communicates with the foramen cecum. Cervical lymphadenopathy may be present if a complicating thyroid cancer is present in a thyroglossal duct anomaly2 (Fig. 202.5).

FIGURE 202.3. An infant presenting with feeding difficulties and a neck mass. The section in the mid neck shows gas present, indicating some connection with a hollow viscus, likely the hypopharynx. This was a surgically proven pharyngeal duplication cyst.
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Cervicothoracic Junction: Brachial Plexus Trauma
Cervicothoracic Junction: Brachial Plexus Trauma
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


