Lisfranc Fracture-Dislocation
Adam T. Ryan
Daniel B. Nissman
CLINICAL HISTORY
Foot pain after jumping off bunk bed.
 FIGURE 44A |
 FIGURE 44B |
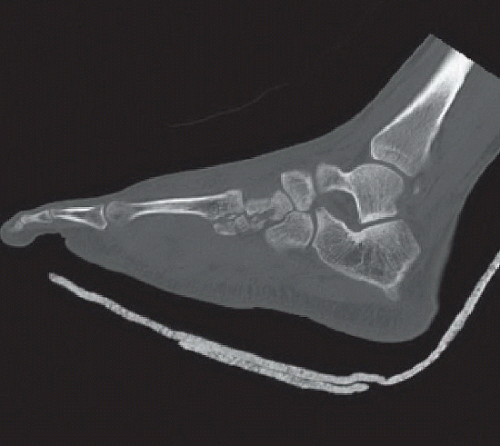 FIGURE 44C |
 FIGURE 44D |
FINDINGS
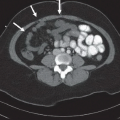
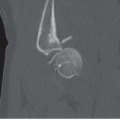
Dorsal-plantar non-weight-bearing radiograph of the right foot (Fig. 44A) demonstrates a subtle incongruity along the medial aspect of the 2nd metatarsal base (black arrow). A weight-bearing dorsal-plantar radiograph was subsequently obtained (Fig. 44B), demonstrating an overt 2nd metatarsal base fracture (white arrow). Sagittal CT image through the second ray (Fig. 44C) demonstrates fractures of the 2nd metatarsal base and middle cuneiform as well as inferior subluxation at the naviculocuneiform joint and dorsal subluxation at the tarsometatarsal (TMT) joint. Dorsal-plantar non-weight-bearing radiograph of the left foot in a different patient (Fig. 44D) demonstrates comminuted fractures of the 1st through 3rd metatarsal bases as well as all three cuneiforms. There is marked lateral displacement of the 2nd through 5th metatarsals and medial displacement of the distal 1st metatarsal fracture fragment. Lateral radiograph
(not shown) revealed dorsal subluxation of the 2nd through 4th metatarsals and dorsal displacement of the 1st metatarsal distal fracture fragment.
(not shown) revealed dorsal subluxation of the 2nd through 4th metatarsals and dorsal displacement of the 1st metatarsal distal fracture fragment.
DIFFERENTIAL DIAGNOSIS
Homolateral Lisfranc fracture-dislocation, divergent Lisfranc fracture-dislocation, Lisfranc ligament avulsion, metatarsal fracture, tarsal bone fracture, Lisfranc ligament injury.
DIAGNOSIS
First case: 2nd TMT joint fracture-dislocation. Second case: divergent Lisfranc fracture-dislocation.
DISCUSSION
Lisfranc fracture-dislocations represent a spectrum of injuries from sprains of the Lisfranc ligament to overt fracture-dislocation of a part or all of the TMT joints. The Lisfranc fracture-dislocation accounts for only 0.2% of all fractures.1 Despite its relative rarity, knowledge of this type of injury is essential to make a timely diagnosis; delayed diagnosis is associated with poor outcomes. A missed diagnosis rate of 20% has been estimated in the emergency department setting.2 Chronic pain, dysfunction from ligamentous instability, arthritis, and deformity are all potential sequelae of delayed or inappropriate treatment.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


