Chapter 3. Liver
Patient Preparation
• Fasting is not required if only the liver is to be evaluated; however, the gallbladder and extrahepatic bile ducts (fasting examinations) are usually included in most evaluations of the liver.
Equipment and Technical Factors
• Because of the depth and breath of the liver, multiple transducer types (sector, vector, curved linear) may be used to thoroughly evaluate the liver. Use of high frequencies to image the anterior surface and left lobe of the liver is recommended. Use of lower frequencies to image the right lobe and diaphragm may be required.
• Technical settings should ensure that the liver parenchyma is a homogenous, midlevel shade of gray with anechoic blood vessels and hyperechoic ligaments, diaphragm, and blood vessel walls.
• Color Doppler imaging may confirm flow in suspected vessels or the hepatic and portal veins and hepatic artery.
Imaging Protocol
• Longitudinal and transverse axis images should be recorded of the functional lobar anatomy: left, right, and caudate lobes. Include all surfaces of the liver, the porta hepatic, hepatic veins, portal veins, and the ligaments, fossa, and fissures.
• Images should be recorded in an efficient, logical, and sequential manner.
• Transverse axis image(s) of the portal triad at the porta hepatis should be included.
• Images may be labeled as Couinaud segments I−VIII as required (surgical resections, transplants).
Variants
• Variations in liver shape and overall size may be noted, including Reidel’s lobe and a small left lobe.
Sonographic Measurements (Normal Limits)
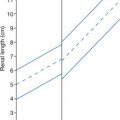
• Cranial to caudal (diaphragm to tip of right lobe) along the midclavicular line: 15.0 cm
• Main portal vein diameter: 13.0 mm
• Other measurements may be performed (may be difficult):
Anterior to posterior through the right lobe: 10.0−21.0 cm
Transverse lateral left lobe through lateral right lobe: 20.0−36.0 cm
• Liver volume: 133.2 + 0.422(CC × AP × LL)
• Right lobe to caudate lobe ratio (from transverse image): diameter of caudate lobe (A) divided by diameter of the right lobe (B); a ratio >0.65 may indicate cirrhosis.
| Liver | |||
|---|---|---|---|
| Sonographic Finding(s) | Clinical Presentation | Differential Diagnosis | Next Step |
Liver measures >15.0 cm along midclavicular line or Extension of right lobe inferior to lower pole of kidney; inferior tip of right lobe may be rounded Left lobe may extend into LUQ | Asymptomatic or Symptoms may be associated with a variety of liver disease states Labs: normal to elevated LFT | Hepatomegaly is associated with a variety of diffuse disease processes: Early cirrhosis Anemia Congestive heart failure Portal hypertension Fatty infiltration Hepatitis Normal variant or the result of patient’s body habitus | Evidence of disease may be subtle May be caused by multiple focal disease: cyst, neoplasm, metastases, abscess Splenomegaly may be present |
Increased echogenicity of liver (mild to significant) with decreased visualization of liver landmarks Mild to severe attenuation of sound Diaphragm difficult to visualize | Usually asymptomatic Possible jaundice, nausea and vomiting, abdominal tenderness/pain Labs: normal to elevated LFT | Fatty infiltration Cirrhosis Hepatitis Metastatic disease | Associated with: ETOH abuse Obesity Pregnancy Severe hepatitis Steroid use Chemotherapy Diabetes Glycogen storage disease Lower transducer frequencies and a variety of scan planes should be used Degree of fatty infiltration may be graded (1–3) |
Patchy area of increased echogenicity near porta hepatis; may be fan shaped, angular, or band shaped No mass effect demonstrated with 2D or color Doppler imaging | Asymptomatic Labs: normal LFT | Focal fatty infiltration | Opposite of focal fatty sparing |
Large liver with increased echogenicity throughout (possibly very echogenic) with area of lesser echogenicity anterior to right portal vein, near porta hepatis or posterior left lobe May at first appear as a “mass”; however, no mass effect is noted | Usually asymptomatic Labs: normal to elevated LFT | Focal fatty sparing | Opposite of focal fatty infiltration |
Normal to hypoechoic liver echogenicity with or without hepatosplenomegaly Prominent portal vein walls may be noted (“starry-sky” appearance) Gallbladder wall thickening may be noted | Flu-like symptoms GI complaints Loss of appetite Low-grade fever Fatigue RUQ pain, jaundice Labs: elevated bilirubin, LDH, ALT, AST, leukopenia | Acute hepatitis: viral (mononucleosis) amebiasis, chemical or drug toxicity | The patient may not be diagnosed with hepatitis before the sonogram May mimic fatty liver |
Normal-sized liver with increased echogenicity (may be brighter than fatty liver) Coarse/heterogenous appearance of liver texture; may be focal or patchy Some attenuation of sound but not as great as fatty liver Decreased brightness of the portal triads | Fatigue Nausea Anorexia Weight loss Jaundice Tremors Varicosities Dark urine Labs: elevated LFT, leukopenia, decreased BUN | Chronic hepatitis: all types except A | Symptoms for 6 months or more May mimic cirrhosis or fatty liver Portal hypertension may be present |
Echogenic mass(es), homogeneous and well defined Round, oval, or lobulated; usually <3.0 cm Posterior enhancement may be noted | Commonly asymptomatic female patient Labs: normal LFT | Typical hemangioma HCC Adenoma Metastasis FNH | Use of power Doppler imaging may demonstrate flow within hemangioma |
Hypoechoic mass or mass with hypoechoic center (reverse target) Variable echogenicity Posterior enhancement or calcifications may be noted
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


| |||