Liver Anatomy
Michael P. Federle, MD, FACR
GROSS ANATOMY
Overview
Largest gland & largest internal organ (average weight = 1,500 grams)
Functions
Processes all nutrients (except fats) absorbed from GI tract; conveyed via portal vein
Stores glycogen, secretes bile
Relations
Anterior & superior surfaces are smooth and convex
Posterior & inferior surfaces are indented by colon, stomach, right kidney, duodenum, IVC, and gallbladder
Covered by peritoneum except at gallbladder fossa, porta hepatis, and bare area
Bare area: Nonperitoneal posterior superior surface where liver abuts diaphragm
Porta hepatis: Site of entry/exit of the portal vein, hepatic artery, and bile duct
Falciform ligament: Extends from liver to anterior abdominal wall
Separates right & left subphrenic peritoneal recesses (between liver & diaphragm)
Marks plane separating medial and lateral segments of left hepatic lobe
Carries round ligament (lig. teres), fibrous remnant of umbilical vein
Vascular supply (unique dual afferent blood supply)
Portal vein
Carries nutrients from gut and hepatotrophic hormones from pancreas to liver along with oxygen (contains 40% more oxygen than systemic venous blood)
75-80% of blood supply to liver
Hepatic artery
Supplies 20-25% of blood
Liver is less dependent than biliary tree on hepatic arterial blood supply
Usually arises from celiac artery
Variations are common, including arteries arising from superior mesenteric artery
Hepatic veins
Usually 3 (right, middle, and left)
Many variations & accessory veins
Collect blood from liver and return it to IVC at confluence of hepatic veins, just below diaphragm and entrance of IVC into heart
Portal triad
At all levels of size and subdivision, branches of hepatic artery, portal vein, and bile ducts travel together
Blood flows into hepatic sinusoids from interlobular branches of hepatic artery & portal vein → hepatocytes (detoxify blood and produce bile) → bile collects into ducts, blood collects into central veins → hepatic veins
Segmental anatomy of liver
8 hepatic segments
Each receives secondary or tertiary branch of hepatic artery and portal vein
Each is drained by its own bile duct (intrahepatic) and hepatic vein branch
Caudate lobe = segment 1
Has independent portal triads and hepatic venous drainage to IVC
Left lobe
Lateral superior = segment 2
Lateral inferior = segment 3
Medial superior = segment 4A
Medial inferior = segment 4B
Right lobe
Anterior inferior = segment 5
Posterior inferior = segment 6
Posterior superior = segment 7
Anterior superior = segment 8
ANATOMY IMAGING ISSUES
Questions
Designating and remembering hepatic segments
Portal triads are intrasegmental; hepatic veins are intersegmental
Separating right from left lobe
Plane extends vertically through gallbladder fossa & middle hepatic vein
Separating right anterior from posterior segments
Vertical plane through right hepatic vein
Separating left lateral from medial segments
Plane of falciform ligament (fissure of ligamentum teres)
Separating superior from inferior segments
Plane of main right & left portal veins
Segments are numbered in clockwise order as if looking at anterior surface of liver
Imaging Pitfalls
Because of variations of vascular & biliary branching within liver (common), it is frequently impossible to precisely designate boundaries between hepatic segments on imaging studies
CLINICAL IMPLICATIONS
Clinical Importance
Advances in hepatic surgery (tumor resection, transplantation) make it essential to depict lobar and segmental anatomy, volume, blood supply, and biliary drainage as accurately as possible
Combination of axial, coronal, sagittal, and 3D imaging by CT, MR, and sonography may be needed
“Invasive” imaging studies (catheter angiography and percutaneous transhepatic or endoscopic cholangiography) can be avoided in many cases by CT & MR angiography and cholangiography
Liver metastases are common
Primary carcinomas of colon, pancreas, & stomach are common
Portal venous drainage usually results in liver being initial site of metastatic spread from these tumors
Primary hepatocellular carcinoma
Common worldwide; usually result of viral hepatitis B or C, alcoholism
Image Gallery
HEPATIC VISCERAL SURFACE
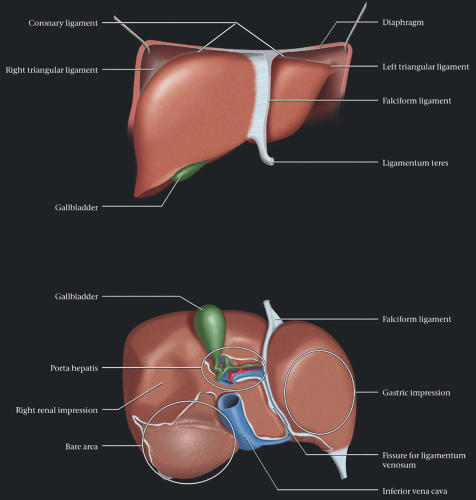 (Top) The anterior surface of the liver is smooth and molds to the diaphragm & anterior abdominal wall. Generally, only the anterior/inferior edge of the liver is palpable on physical exam. The liver is covered with peritoneum, except for the gallbladder bed, porta hepatis, and the bare area. Peritoneal reflections form various ligaments that connect the liver to the diaphragm & abdominal wall, including the falciform ligament, the inferior edge of which contains the ligamentum teres, and the obliterated remnant of the umbilical vein. (Bottom) Graphic shows the liver inverted, somewhat similar to the surgeon’s view of the upwardly retracted liver. The structures in the porta hepatis include the portal vein (blue), hepatic artery (red), and bile ducts (green). The visceral surface of the liver is indented by adjacent viscera. The bare area is not easily accessible. |
HEPATIC ATTACHMENTS AND RELATIONS
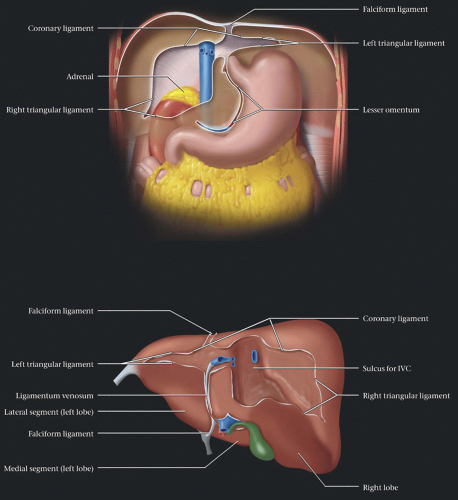 (Top) Liver is attached to the posterior abdominal wall and diaphragm by the left & right triangular and the coronary ligaments. The falciform ligament attaches the liver to the anterior abdominal wall. The bare area is in direct contact with the right adrenal & kidney, and the IVC. (Bottom) Posterior view of the liver shows the ligamentous attachments. While these may help to fix the liver in position, abdominal pressure alone is sufficient, as evidenced by orthotopic liver transplantation, after which the ligamentous attachments are lost without the liver shifting position. The diaphragmatic peritoneal reflection is the coronary ligament, which has the right & left triangular ligaments as its lateral extensions. The falciform ligament separates the medial & lateral segments of the left lobe. |
HEPATIC VESSELS AND BILE DUCTS
 This graphic emphasizes that, at every level of branching and subdivision, the portal veins, hepatic arteries, and bile ducts course together, constituting the “portal triad.” Each segment of the liver is supplied by branches of these vessels. Conversely, hepatic venous branches lie between hepatic segments and interdigitate with the portal triads, but never run parallel to them. |
HEPATIC SEGMENTS
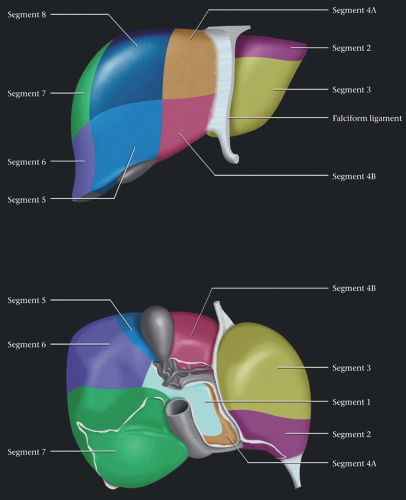 (Top) This is the 1st of 2 graphics demonstrating the segmental anatomy of the liver in a somewhat idealized fashion. Segments are numbered in a clockwise direction, starting with the caudate lobe (segment 1), which cannot be seen on this frontal view. The falciform ligament divides the lateral (segments 2 & 3) from the medial (segments 4A & 4B) left lobe. The horizontal planes separating the superior from the inferior segments follow the course of the right and left portal veins. An oblique vertical plane through the middle hepatic vein, gallbladder fossa, and IVC divides the right & left lobes. (Bottom) Posterior view of the liver shows that the caudate is entirely posterior, abutting the IVC, ligamentum venosum, & porta hepatis. A plane through the IVC and gallbladder divides the left & right lobes. |
AXIAL CT, NORMAL LIVER
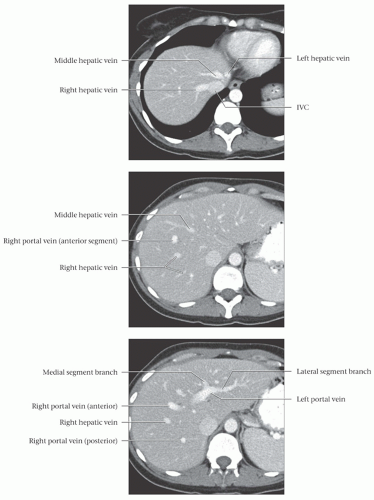 (Top) This is the 1st of 9 axial CT sections. This image shows the confluence of the hepatic veins with the IVC just below the diaphragm and the entrance of the IVC into the right atrium. (Middle) At this level, the portal veins run in a predominantly cephalo-caudal direction and bisect the angle made by the hepatic veins. Portal veins generally lie within hepatic segments, while hepatic veins lie between segments. (Bottom) The horizontal plane, defined by the left portal vein, divides the lateral segment into segment 2 (above the vein) and 3 (below). |
AXIAL CT, NORMAL LIVER
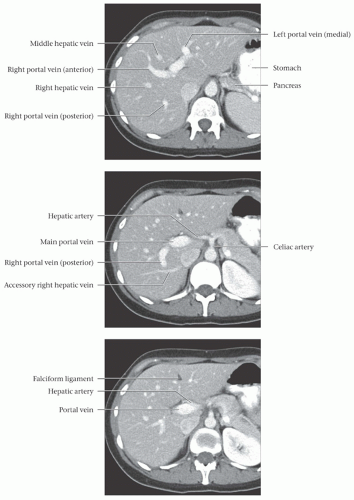 (Top) The plane of section through the long axis of the right portal vein divides segments 7 & 8 (above) from segments 5 & 6 (below). Note the relations between the liver, stomach, and pancreas. (Middle) In this subject, the hepatic artery arises conventionally from the celiac artery. There is an accessory right hepatic vein that drains directly into the IVC, caudal to the confluence of the other hepatic veins. This accessory vein may have important implications in the setting of partial liver resection or transplantation. (Bottom) Note the fissure for the falciform ligament (ligamentum teres), which separates the medial and lateral segments of the liver (segment 4 from segments 2 and 3).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|