The Liver
Normal Liver
Normal Anatomy
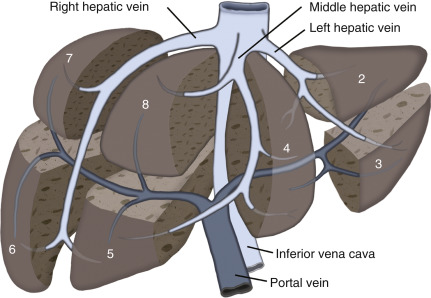
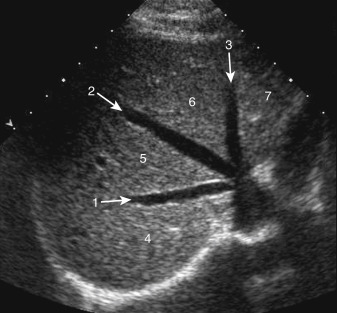
The cephalad portion of the liver is bounded by the diaphragm. The caudal extent of the liver is in close proximity to the stomach, the duodenum, and the large bowel and lies just cephalad to the pancreas. Using the Couinaud classification of liver anatomy, the liver is divided into eight segments. Segment 1 is the caudate lobe. The caudate’s boundary is the inferior vena cava (IVC) posteriorly and the portal vein and the echogenic fissure of the ligamentum venosum more anteriorly. The main lobar fissure, which extends from the gallbladder to the middle hepatic vein, divides the right from the left lobe of the liver ( Fig. 16.1 ). Knowledge of the location of the main lobar fissure is useful to locate the gallbladder, especially if the gallbladder is contracted or is full of stones. The gallbladder lies in the caudal extent of the main lobar fissure. The left lobe contains segments 2, 3, and 4A and 4B; the right lobe contains segments 5, 6, 7, and 8. The ligamentum teres is an easily identifiable landmark, which is the fibrous remnant of the umbilical vein. It separates segment 3 and segment 4B of the left lobe. The left hepatic vein can be thought of as the more cephalad extension of the ligamentum teres and divides segment 2 and segment 4A of the left lobe of the liver. The right hepatic vein divides the more posterior segments 6/7 from the more anterior segments 5/8 of the right lobe ( Figs. 16.1 and 16.2 ).
The common hepatic artery usually arises from the celiac artery and passes as the proper hepatic artery anterior to the portal vein. Common hepatic artery variants include the right hepatic artery arising from the superior mesenteric artery and passing posterior to the portal vein as a replaced right hepatic artery. There are a number of variants of the origin and branches of the hepatic artery, including a replaced or accessory left hepatic artery. Most of these variants are not easily visualized with ultrasound (US).
Ultrasound Findings/Technique
When scanning the liver, multiple transverse and longitudinal scans are obtained with the patient supine. Usually the liver is scanned with a curved array transducer with center frequency from 3 to 5 MHz. Higher-frequency linear array transducers may be used to examine the liver surface to assess for cirrhotic nodules.
The subcostal approach may be used for visualization of the right lobe, especially if the patient can hold a deep inspiration. Portions of the right lobe of the liver will require the patient to be placed in the right anterior oblique position. Using this technique, it is important to place the transducer parallel to the intercostal space. If this is not done, there will be acoustic shadowing from adjacent ribs, which prevents good visualization of the liver. The transducer often must be angled in a cephalad direction to scan the majority of the right lobe of the liver. Scanning performed intercostally may be helpful to identify the subdiaphragmatic portion of the liver, such as segments 7 and 8. Unfortunately, it may be difficult to visualize all portions of the right lobe of the liver because of the shadowing by the lung. This is why scanning in the intercostal space with the right side of the abdomen elevated is important. The left lobe can be scanned using an anterior subxiphoid approach.
Normally, the liver appears as a homogeneous structure, with echogenicity slightly greater than or equal to the kidney. This internal comparison is important, as with increasing hepatic steatosis there will be increasing echogenicity of the liver. The homogeneous echogenicity is only interrupted by the portal triads and the hepatic veins. The size of the liver is variable, with the length of the right lobe of the liver varying between 13 and 17 cm. Liver volume is not usually calculated, and there is considerable variability in the size of the right and left lobes of the liver.
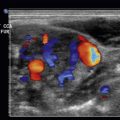
Color Doppler ultrasound is important to use to identify the portal vein and its normal direction of hepatopetal flow (toward the liver). In patients with cirrhosis, the portal vein can increase in size. Eventually there can be hepatofugal (reversed) flow in the portal vein. Color flow may be helpful to identify any thrombus in the portal vein. Pulsed Doppler ultrasound is used to identify the direction of flow in the portal vein. Color flow in the hepatic veins is easily obtained and is helpful to exclude occlusion of the hepatic veins. Pulse Doppler may be used to identify the normal triphasic hepatic waveform. The IVC can be identified posterior to the liver and heading anteriorly to the right atrium. The hepatic artery can be seen with color and noting its arterial waveform with pulsed Doppler.
Liver: Etiologies of Right Upper Quadrant Pain
Hepatic Cysts
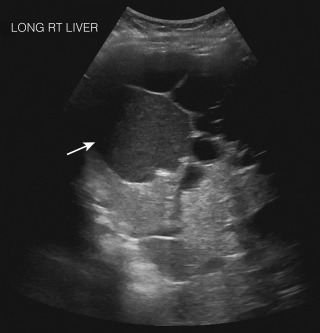
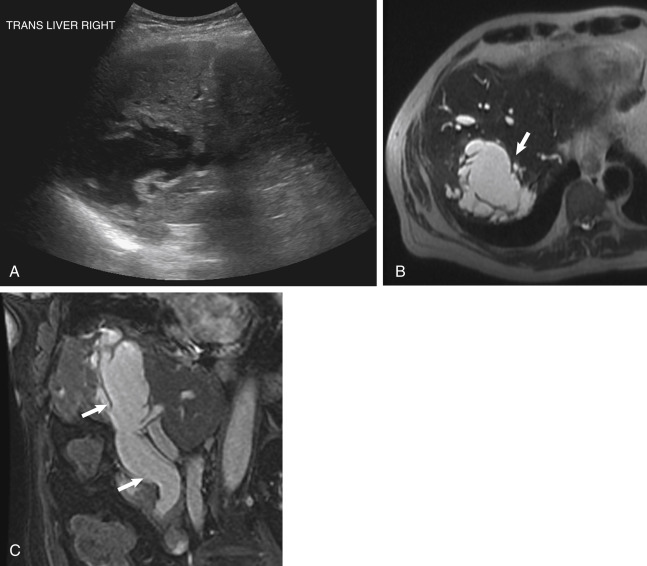
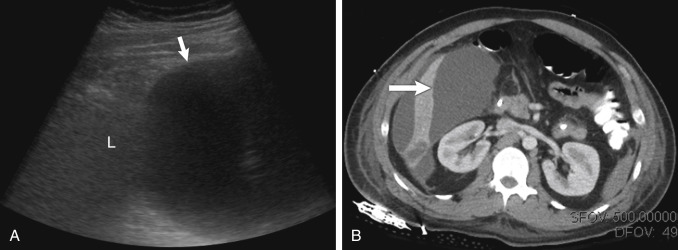
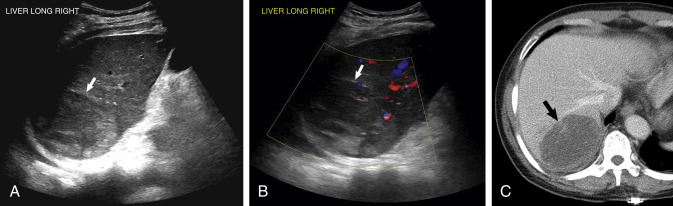
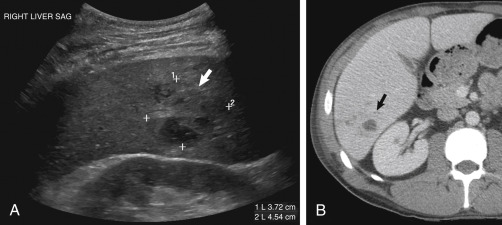
A hepatic cyst is rarely the etiology of right upper quadrant (RUQ) pain, unless it is large enough to distort the liver capsule or it has hemorrhaged internally. Cysts are anechoic with smooth walls with good through transmission. Cysts with avascular septations or debris are called complex cysts . Upper abdominal pain may occur with hemorrhage into a hepatic cyst. Cysts with internal hemorrhage may become echogenic, appear more complex, or have a fluid/blood interface ( Fig. 16.3 ). Although a complex cyst may be due to hemorrhage, the differential for a complex hepatic cyst is fairly broad ( Fig. 16.4 ). The differential can include anything from a postoperative or posttransplant hematoma to postoperative seroma or biloma ( Fig. 16.5 ). Historical information is important in narrowing the ultrasound differential. Rarer causes of more complex hepatic cysts are listed in Table 16.1 . If a complex cyst is encountered, computed tomography (CT) or magnetic resonance imaging (MRI) may be useful for better characterization.
| Hemorrhagic cyst | Pseudoaneurysms (use color flow) |
| Infected cyst | Polycystic renal disease (multiple hepatic cysts) |
| Biloma | Multiple hepatic cysts |
| Abscess | Mucinous (cystic) biliary tumor |
| Echinococcal cyst | |
| Necrotic hepatic tumor |
Abscess
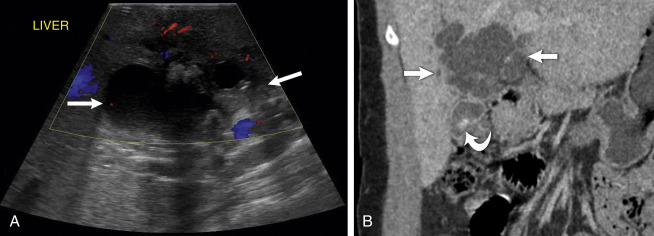
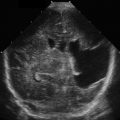
Bacterial liver abscesses are an etiology of acute abdominal pain. Bacterial abscesses are usually hypoechoic but may be isoechoic or echogenic ( ![]() ). They may have thick or poorly defined walls ( Figs. 16.6 and 16.7 ). They may be difficult to diagnose on ultrasound. Therefore the clinical presentation is helpful. Again, CT or MRI may be needed to better characterize an hepatic abscess. Liver abscesses may be secondary to infection from adjacent structures, such gallbladder perforation into the liver from acute cholecystitis ( Fig. 16.8 ,
). They may have thick or poorly defined walls ( Figs. 16.6 and 16.7 ). They may be difficult to diagnose on ultrasound. Therefore the clinical presentation is helpful. Again, CT or MRI may be needed to better characterize an hepatic abscess. Liver abscesses may be secondary to infection from adjacent structures, such gallbladder perforation into the liver from acute cholecystitis ( Fig. 16.8 , ![]() ). An hepatic abscess may also occur from hematogenous spread due to acute diverticulitis or appendicitis. It is important to realize that although abscesses often appear complex with thick internal separations, they may also appear solid and could be confused with a solid mass (see Figs. 16.6 and 16.7 ).
). An hepatic abscess may also occur from hematogenous spread due to acute diverticulitis or appendicitis. It is important to realize that although abscesses often appear complex with thick internal separations, they may also appear solid and could be confused with a solid mass (see Figs. 16.6 and 16.7 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


